Epilepsy linked to meningioma - Physiopathology, predictors and treatment of pre/postoperative crises
by Rasha Elbadry Ahmed1 †, Hailiang Tang2 †, Anthony Asemota1, lei Huang1,3, Warren Boling1*‡ and Firas bannout4*‡
-1 Neurosurgery, Loma Linda University Medical Center, Loma Linda, CA, United States
- 2 Neurosurgery, Huasha Hospital, Fudan University, Shanghai, China
-3 Between physiology and pharmacology, University of Loma Linda, Loma Linda, CA, United States
-4 Neurology departure, medical center of the University of Loma Linda, Loma Linda, CA, United States
Les méningiomes sont les tumeurs cérébrales primaires les plus courantes et représentent environ 30 % de toutes les tumeurs cérébrales. La grande majorité des méningiomes ont une croissance lente et une histopathologie bénigne, ce qui les rend curables par la seule chirurgie.
Symptomatic lesions depend on their location with signs of mass effect or neurological deficits.
Epilepsy attacks are the main symptom in around 30 % of cases, which negatively affects quality of life, limits independence, alters cognitive functioning and increases the risk of psychiatric comorbidities, including depression.
Bien que la résection chirurgicale puisse offrir une absence de crises dans 60 à 90 % des méningiomes, les crises persistent après la résection chirurgicale chez environ 12 à 19 % des patients.
Anti-convulsion drugs (ASM) are used in management, but they are limited by unwanted neurocognitive side effects and their ineffectiveness in certain patients.
Potential predictors of pre -and postoperative crises in patients with meningioma have been identified in the literature.
Understanding the various factors associated with the probability of crises in patients with meningiomal can help guide more effective control of crises and allow better risk determination before and after surgery.
Introduction
Les méningiomes représentent environ 30 % des tumeurs cérébrales primaires et approximativement 54% des tumeurs bénignes primaires (1-3). La grande majorité des méningiomes sont d’évolution lente et d’histopathologie bénigne (c’est-à-dire des tumeurs de grade I de l’Organisation mondiale de la santé (OMS)), ce qui les rend curables par la seule chirurgie (4, 5). Les lésions symptomatiques dépendent de leur localisation avec des signes d’effet de masse ou des déficits neurologiques. Les crises d’épilepsie sont le symptôme initial dans environ 30 % des cas, et dans certaines études, le pourcentage varie de 13 à 60 % (6-8). Bien que la résection chirurgicale puisse offrir une absence de crises dans 60-90 % des méningiomes, les crises peuvent persister après la résection chirurgicale chez environ 12-19 % des patients (9, 10). Les crises peuvent avoir un impact négatif sur la qualité de vie, en entravant l’indépendance du patient, ses fonctions cognitives et sa capacité à conduire en toute sécurité (11-13). Elles exposent les patients à un risque accru de différentes comorbidités psychiatriques, dont la dépression (14). Le contrôle des crises à l’aide de divers médicaments anti-crises (ASM) est généralement proposé malgré les effets secondaires indésirables sur la neurocognition et l’inefficacité chez certains patients (15).
De nombreuses théories ont été avancées pour expliquer la pathogenèse de l’épilepsie liée aux tumeurs cérébrales (BTRE) dans diverses tumeurs cérébrales ; cependant, des questions restent sans réponse concernant le contrôle et la gestion des crises chez les patients atteints de méningiomes, par exemple, la capacité des résections chirurgicales à guérir les crises, quand commencer les ASM, la durée du traitement ainsi que des directives structurées pour la sélection des patients pour les ASM. Comprendre et prédire les crises dans les méningiomes peut aider à guider le contrôle des crises et permettre de mieux déterminer les patients à risque avant et après la chirurgie. Cette revue a pour but de résumer la pathogenèse des crises dans les méningiomes, les facteurs prédictifs pré et postopératoires des crises, la résection chirurgicale qui permet d’éliminer les crises, les avantages de l’utilisation des ASM, l’électrocorticographie (ECoG) peropératoire et la surveillance de l’électroencéphalogramme (EEG) chez les patients atteints de méningiomes et la sélection adéquate des patients.
Incidence of epilepsy in meningiomas
L’incidence des crises préopératoires dans le cas des méningiomes a été rapportée respectivement à 29 % sur 4709 patients (7) et à 14 % sur 598 patients (16) atteints de méningiomes supratentoriels.
L’absence de crises a été obtenue chez environ 69 % des patients après la chirurgie, avec 12 % de nouvelles crises survenant après la chirurgie (17). L’étude de Chozick a rapporté que 63/158 patients atteints de méningiome avaient des crises préopératoires et que 40 (63,5 %) des 63 patients avaient une résolution complète des crises après la chirurgie dans les années de suivi de 7,3± 3,8. Dans cette cohorte, 100 % des 63 patients étaient sous traitement anticonvulsivant avant l’opération et pendant la phase initiale postopératoire. Les auteurs n’ont pas indiqué la proportion exacte de ces 43 patients sevrés de médicaments anticonvulsivants au fil du temps postopératoire. Alors que certains neurochirurgiens avaient tendance à cesser d’utiliser les médicaments environ 6 mois après l’opération s’il n’y avait aucun signe de crises, les autres neurochirurgiens ont continué à utiliser les anticonvulsivants à titre prophylactique. Ils ont rapporté que quatre-vingt-cinq patients (53,8 % des 158) ont finalement été sevrés d’anticonvulsivants et que 44,7 % d’entre eux n’avaient pas cessé d’en prendre lors de la dernière visite de suivi postopératoire. Les crises sont réapparues chez un patient pendant le processus de sevrage des ASM, chez 4 patients avec des niveaux d’ASM sous-thérapeutiques, chez 6 patients qui n’étaient pas sous ASM, chez 2 patients corrélés à l’abus d’alcool et chez 5 patients avec une récidive tumorale. Huit patients (5,1%) sans antécédents d’épilepsie préopératoire ont développé des crises postopératoires. Chozick et al. ont conclu que dans leur étude, seule l’étendue de l’ablation de la tumeur était un facteur prédictif significatif de crises postopératoires.
However, history of preoperative epileptic crisis, preoperative language disorders, postoperative status of anti-crisis drugs, postoperative hydrocephalus or the location of tumor in the parietal region were also predictive factors for the occurrence of postoperative epileptic crises (18). Wirsching reported 26.6 % postoperative crises during a median period of 67 months (95 % CI: 63-72) postoperative monitoring (19).
The great variation of these studies can be due to the lack of standardization of the data collected retrospectively in patients with different demographic characteristics, characteristics/locations/types of different meningiomas, different monitoring periods, analyzes of different age groups between pediatric and adult patients, and different surgical skills and techniques in different institutions. The majority of postoperative crises were felt during the first week after the operation, but a third of patients presented crises three months after the operation (17).
Pathogenesis of epilepsy linked to meningioma
The pathophysiology of epilepsy linked to a brain tumor is multifactorial and can be divided into morphological, biochemical and metabolic causes.
The morphological changes in the peritumoral neocortex include the connection of neurons and the connectivity and location of synaptic vesicles, resulting in a higher concentration of NA+ voltage channels, Ca ++ and glutamate receptors with a loss of inhibitory synapses and an increase in excitatory synapses. Biochemically, there is an increase in glutamatergic neurons and a reduction in immunoreactive gabaergic neurons to somatostatin. At the ionic level, we observe a low rate of MG2+, a high rate of extracellular K+, a high rate of Fe3+, a low rate of K+/Cl- Cotransporter-2 (KCC2) specific to neurons. It is believed that the peritumoral extracellular pH is slightly alkaline. Finally, there are enzymatic changes, amino and immunological acids with upward regulation of glutamatergic receptors for neurotransmitters NMDA and AMPA (24).
More recently, the genetic factors of the epileptogenicity of meningiomas have been studied. The NF2 mutation has proven to be a predictive marker of preoperative crises, via an indirect mediation effect with atypical histology and edema (25). Meningioma comes from cells in the arachnoid cap and is generally a slow growth tumor (1). This slow growth can partly explain the peritumoral modifications which lead to epileptogenicity (24, 26). Partial differentiation of the cortical surface of the brain can produce an epileptogenic area, thus causing denervation hypersensitivity (27). The morphological changes that develop in the cerebral fabric adjacent to the lesion, such as ineffective neuronal migration, synaptic vesicles and alterations of the Gap-Junction Glial coupling, are also supposed to contribute to the generation of crises (28). Although pediatric meningiomas are rare, epilepsy has been reported as one of the current symptoms (29). A ineffective neuronal migration could constitute an additional peritumoral mechanism of epileptogenesis in this age group of patients.
Le pourcentage d’œdème cérébral chez les patients atteints de méningiome varie entre 30 et 60 % (30-32). Il est généralement vasogénique et lié à une augmentation de l’apport pial, à l’angiogenèse et à l’expression accrue du facteur de croissance endothélial vasculaire (VEGF) (33, 34). Les modifications chimiques du milieu péritumoral et l’hypoxie locale due à la compression locale de la tumeur sont considérées comme des mécanismes sous-jacents qui diminuent le seuil des crises (26). L’augmentation des niveaux de glutamate dans l’œdème péritumoral est souvent décrite comme un facteur instigateur de l’état d’hyperexcitabilité et d’épilepsie (8, 26).
L‘œdème est fortement corrélé à l’invasion du cerveau (35), et peut également être intimement associé à la localisation de la tumeur et à des méningiomes plus invasifs et de grades plus élevés (31, 32, 36). Notamment, Hess et al. ont rapporté une multiplication par cinq du volume de l’œdème chez les patients présentant une invasion cérébrale par rapport à ceux n’en présentant pas, avec une augmentation de 20 % du risque d’invasion cérébrale pour chaque augmentation de 1cm de l’œdème péritumoral (35). Chernov, et al. ont rapporté une incidence élevée d’œdème péritumoral dans les méningiomes invasifs macroscopiques (37). L’invasion cérébrale et la rupture de la couche arachnoïde déforment et altèrent le cortex péritumoral, libérant des acides aminés et affectant la voie des neurotransmetteurs (35, 38).
En ce qui concerne l’apparition de crises postopératoires, les fortes adhésions peropératoires, la nécessité de procéder à une microdissection, ainsi que les éventuelles lésions de la surface corticale et l’irritation peuvent contribuer à la génération, en particulier chez les patients n’ayant jamais eu de crises (36). La rétraction et la manipulation, qui sont parfois nécessaires pour obtenir une résection totale dans les lésions de la base du crâne, peuvent également entraîner des lésions corticales supplémentaires et un œdème (39). Les complications postopératoires telles que l’infection, l’hématome et l’hydrocéphalie peuvent encore accroître l’œdème cérébral et augmenter le risque de crises (40).
Based on histopathological characteristics, the WHO classification system classifies meningiomas in Grade I (Benin), Grade II (atypical) and Grade III (anaplastic) (41). Hess et al. have retrospectively analyzed the cerebral invasion and the risk of convulsions in a total of 176 patients with meningiomas. There were 92 (52 %) Grade I, 79 (45 %) tumors of Grade II, and 5 (3 %) of Grade III. Grade I meningiomas included 16 (17 %) transitional subtypes, 4 (4 %) secretory, 68 (74 %) meningothelial, 3 (3 %) fibrous and 1 (1 %) angiomatous. Preoperative crises were present in 10 (11 %) of the 92 patients with grade I, 23 (29 %) of the 79 patients with grade II meningioma, and absent in patients with anaplastic meningioma. In the meningiomas of Grade I, the histopathological subtype was significantly correlated at the rate of preoperative epilepsy. Overall, the risk of preoperative epileptic crisis was significantly higher in patients with a tumor of grade II or III than in those with a grade I tumor. Brain invasion was absent in all patients with grade I meningioma, but it was present in 35 (44 %) of patients with atypical meningioma and in 3 (60 %) Anaplastic meningioma.
The brain invasion was independent of the volume of the tumor but strongly correlated with the volume of the edema. Multivariate analyzes have shown that the risk of preoperative crises was much higher in patients with meningioma with cerebral invasion than in those with non-invasive meningioma (OR 5.26, 95 % 1.52-18.15 CI; p = 0.009).
Cependant, les taux d’absence de crises postopératoires étaient similaires chez les patients atteints de méningiome invasif et ceux atteints de méningiome non invasif. L’incidence de l’épilepsie postopératoire était corrélée de manière significative avec l’augmentation du volume tumoral préopératoire (35). Dans une autre étude rétrospective, Gadot et al. ont examiné les 384 patients qui ont subi une résection de méningiome. L’association significative n’a pas été trouvée entre un sous-type histologique et de plus mauvais résultats postopératoires en matière de crises d’épilepsie. Cependant, il y avait une tendance associative entre les sous-types de grades plus élevés (malin, rhabdoïde) avec de plus mauvais résultats postopératoires en matière de crises. Les sous-types de grades inférieurs (fibreux, transitionnel) avaient tendance à améliorer les résultats postopératoires (p = 0,081) (25). Il n’existe pas de données dans la littérature médicale pour les petits méningiomes fortuits, qui ne font pas partie du réseau épileptogène.
Predictive factors of epilepsy in the case of meningioma
In order to better understand and predict epilepsy attacks in patients with meningioma, several retrospective studies have examined the possible predictors of crises both preoperatively and postoperatively. Throughout the literature, peritumoral edema and the location were associated with crises in meningiomas. Peritumoral edema has been the subject of in -depth studies and is considered to be the strongest predictor of crisis both preoperatively and postoperatively (7, 8, 17, 20, 21, 26, 35). The probability of obtaining an absence of a postoperative crisis is less in patients with significant preoperative edema (21, 42).
Predictive predictive factors
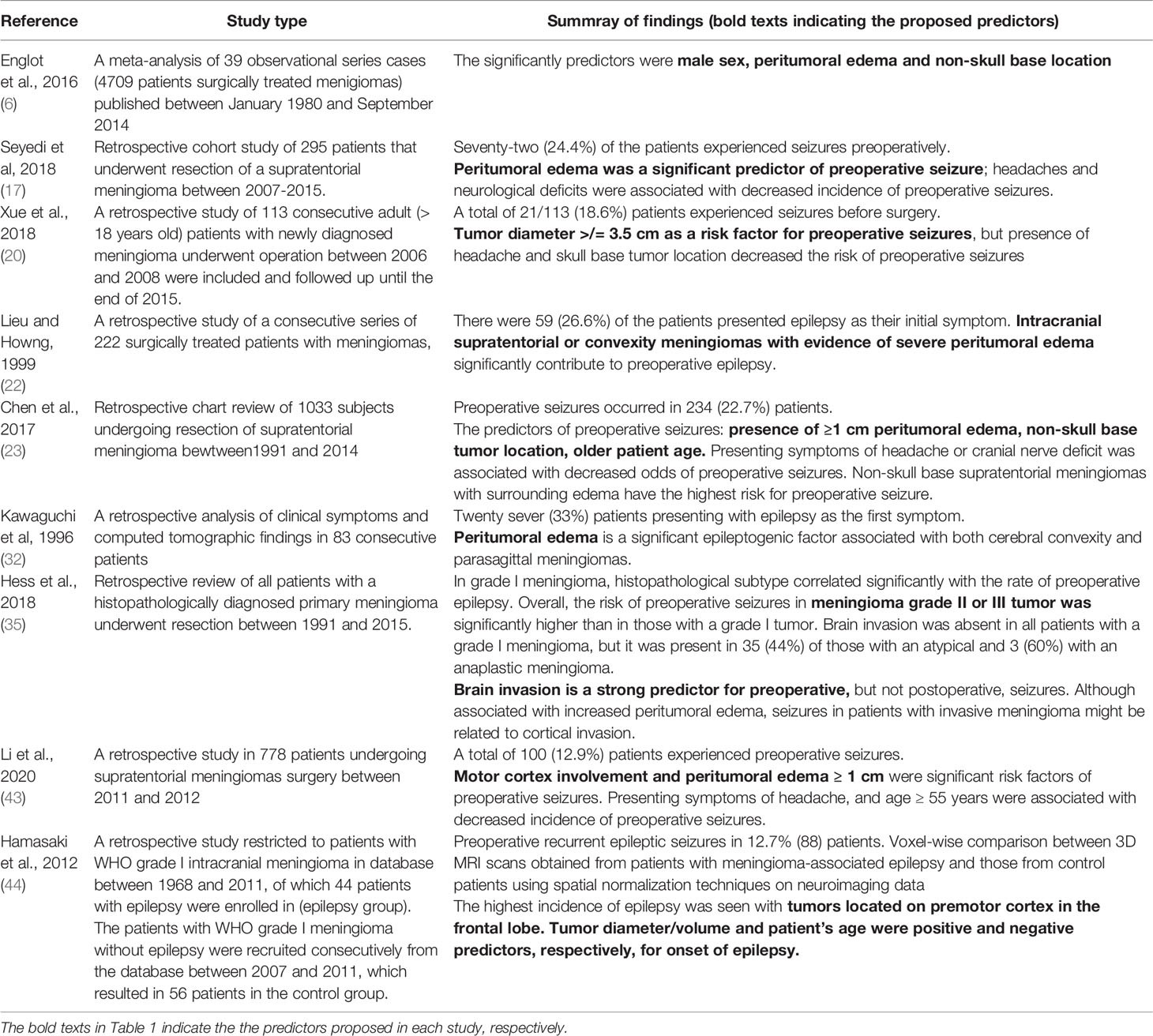
The predictive predictive factors of epilepsy/convulsions are summarized in Table 1.
Table 1
Tableau 1 Facteurs prédictifs de l’épilepsie/crises préopératoires.
Dans une étude rétrospective de Li et al. L’œdème péritumoral de > 1cm était parmi les facteurs de risque identifiés pour les crises préopératoires chez les patients atteints de méningiome (43). La localisation de la tumeur dans les lobes temporal, pariétal et frontal (adjacent au néocortex) est plus susceptible d’être associée à des crises (7, 18, 20, 21). Plus précisément, Lieu et Howng ont noté que la tumeur située dans le lobe temporal augmentait le risque de crises préopératoires par rapport aux autres lobes. On pense que l’augmentation de l’œdème péritumoral remarqué dans les méningiomes convexes et parasagittaux favorise la probabilité d’une augmentation de la fréquence des crises chez les individus affectés. Les méningiomes qui ne sont pas à la base du crâne sont suggérés comme étant plus agressifs avec un indice MIB élevé (pourcentage de cellules tumorales immunoréactives) qui favorise l’invasion du cerveau, l’œdème et les crises (20, 45). Dans une autre étude, aucun consensus n’a été trouvé concernant la zone corticale la plus épileptogène (46).
La plupart des études suggèrent que des tumeurs plus grosses sont naturellement associées à un risque plus élevé de crise préopératoire. Il est concevable que des tumeurs plus grandes puissent causer plus d’irritation et de compression sur les tissus cérébraux environnants. Des résultats similaires rapportés par Chen et al. ont montré que les tumeurs de plus de 3 cm, de grade supérieur avec un œdème péritumoral de plus de 1 cm sont associées à des crises préopératoires (20). Dans une étude, aucune corrélation statistiquement significative entre la taille de la tumeur et les crises préopératoires n’a pu être trouvée (43), alors que le diamètre moyen de la tumeur de 3,5 cm a été utilisé comme seuil pour démontrer une association avec les crises postopératoires à l’hôpital.
Il est intéressant de noter que les méningiomes sont plus fréquents chez les femmes, mais que les hommes sont plus susceptibles de présenter des crises d’épilepsie. De nombreuses études ont montré que le sexe masculin est un facteur de risque de développer des crises préopératoires (7, 8, 20, 23, 43). Il existe une association possible entre le sexe masculin et un méningiome de grade plus élevé, une taille plus grande et un œdème plus important (20). Un âge plus jeune était un facteur prédictif (44), et une incidence plus faible de crises préopératoires a été trouvée chez les patients atteints de méningiomes âgés de plus de 55 ans (43).
Other factors such as preoperative Karnofsky (KPS) have also been studied. A KPS <80 was positively associated with preoperative crises (40). Englot et al. reported a reduced impact of preoperative crises in patients with cranial nerves deficits (7). However, studies on the frequency of symptoms have limits. Prospective studies are necessary to validate these potential predictors.
Postoperative predictors
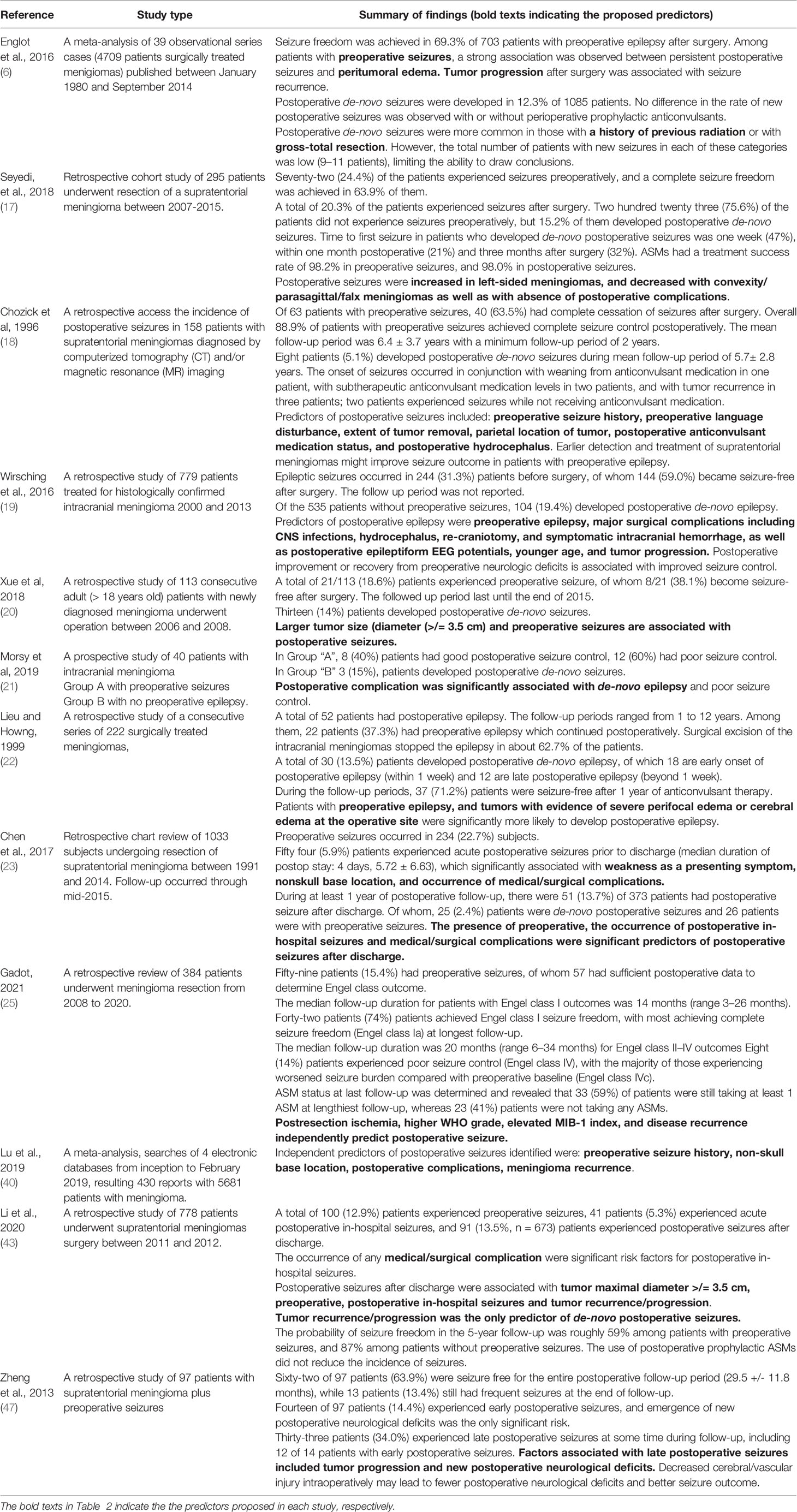
Postoperative epilepsy/convulsions predictors are summarized in Table 2.
Table 2
Tableau 2 Prédicteurs de l’épilepsie/des crises postopératoires.
The International League against Epilepsy (LIG) defined acute postoperative crises as crises occurring within seven days of craniotomy (48). The late postoperative crisis is defined as an epilepsy crisis occurring beyond the first week of surgery (21, 49). In a retrospective study on 556 patients who underwent meningioma surgery, 74 patients presented postoperative crises, including 43% late crises (49). Certain studies have categorized postoperative crises in early, late crisis, in hospital and after leaving the hospital. The identification of possible predictors of postoperative crises can help guide the control of crises and to minimize the complications associated with the long -term use of ASM (13, 17, 20, 43, 47, 50).
La localisation de la tumeur, sa taille, son grade, l’atteinte de la zone motrice et le KPS ont tous été étudiés comme facteurs prédictifs de crises postopératoires (21, 23). Dans une étude, la survenue de crises précoces à l’hôpital était associée à l’implication du cortex moteur, à un KPS postopératoire < 70, à des complications postopératoires et à des crises préopératoires (43). Il a été suggéré que la diminution du seuil et l’augmentation de la sensibilité du cortex pendant la période postopératoire immédiate sont des facteurs importants à prendre en compte, et que l’utilisation des ASM peut être justifiée pendant cette période. Le KPS < 80 était un prédicteur indépendant de crises postopératoires, avec un risque presque trois fois plus élevé d’avoir des crises préopératoires (40). Ceci explique encore l’impact des crises sur la qualité de vie. Les lésions de la base du crâne ont été associées à une diminution de l’incidence des crises en préopératoire, avec une tendance opposée et une incidence accrue en postopératoire (40). Chen et al, dans une étude portant sur 1033 patients, ont rapporté une diminution de l’incidence des crises dans les lésions de la base du crâne (20). Les lésions de la base du crâne nécessitent une plus grande rétraction du cerveau, ce qui augmente encore l’œdème cérébral (7, 51). Scott et al. ont noté une association entre le méningiome du côté gauche et un plus grand risque de développer des crises (52), avec des taux plus élevés de crises postopératoires rapportés dans l’hémisphère gauche (66,7%) par rapport à l’hémisphère droit (23,3%) (17). Dans une étude radiologique analysant l’imagerie par résonance magnétique (IRM) structurelle en 3D de patients atteints de méningiomes afin d’identifier les points chauds pour les crises, les résultats ont montré une probabilité élevée de crises lorsque la lésion était située sur le cortex moteur du lobe frontal (44).
Les crises préopératoires étaient de forts prédicteurs de crises postopératoires, en particulier de crises non contrôlées (13, 17, 20, 43). Il y a une contradiction dans la littérature concernant les déficits neurologiques comme symptômes de présentation. Dans certaines études, il était associé à une moindre incidence de crises préopératoires (17, 20), et dans d’autres, il s’est avéré être significativement associé à des crises postopératoires avant la sortie (10, 19). Lors d’une analyse univariée, Chen et al. ont constaté qu’un déficit neurologique sous la forme d’une nouvelle faiblesse, d’une pneumonie, d’un hématome et d’un infarctus avec œdème était significativement associé à des crises à l’hôpital. Dans leur étude, la faiblesse était un facteur prédictif de crises à l’hôpital mais pas avant ou après la sortie de l’hôpital (20). Il est intéressant de noter que Wirsching et al. ont constaté que l’amélioration postopératoire et la récupération des déficits neurologiques préopératoires étaient associées à un risque plus faible de crise postopératoire et à un meilleur contrôle (19).
Les complications postopératoires sont des prédicteurs indépendants de crises postopératoires (20). Dans la période postopératoire immédiate, le cerveau est plus sensible et son seuil de convulsion est abaissé (43). Toute irritation du néocortex très sensible et probablement encore œdémateux peut aggraver les crises immédiatement après la chirurgie. Une corrélation positive a été établie entre les complications postopératoires comme l’hématome, l’hydrocéphalie, l’infection et l’œdème (40). De nouveaux déficits neurologiques postopératoires permanents, en particulier chez les patients présentant des lésions vasculaires, ont augmenté de manière significative le risque de crises postopératoires (47). Wirshing et al. ont spécifié les complications chirurgicales majeures comme les infections du système nerveux central, l’hydrocéphalie, la re-craniotomie et l’hémorragie intracrânienne symptomatique comme facteurs de risque de crises postopératoires (19).
For crises after leaving the hospital, Li et al. identified the size of the tumor> 3.5 cm, preoperative crises and the progression of the tumor as important predictors (43). In the same study, postoperative complications were associated with acute postoperative crises, but no correlation with postoperative crises during long -term follow -up. In another study, surgical complications were associated with hospital crises and crises after leaving the hospital in patients who have never had crises (19, 53). Chen et al. did not find that tumor recurrence or subtotal resection were important predictors of postoperative crises (20). Englot et al. found a strong association between the deficits of the cranial nerves and the crises after leaving the hospital during a univariate analysis (7).
Surgical resection and freedom of epilepsy
L’amélioration des techniques chirurgicales et le diagnostic plus précoce du méningiome ont eu une incidence sur l’étendue de la résection avec des résultats favorables. Comme indiqué précédemment, la chirurgie permet d’éliminer les crises d’épilepsie chez 70 % des patients, avec des taux allant de 19 % à 90 % (7, 21). Dans certaines études, la liberté globale de crise sur un suivi de 5 ans était de 87% chez les patients ayant des crises préopératoires et de 59% chez les patients naïfs de crises (4, 43). Lu et al. ont rapporté un taux de 30-40% de crises postopératoires chez les patients ayant des antécédents de crises avant l’opération et 10-15% chez les patients naïfs de crises (40). Komotar et al. ont montré une influence significative de la résection totale brute sur les taux de crises (54). Ces rapports soutiennent l’intervention chirurgicale et la cytoréduction chez les patients présentant des crises persistantes. En revanche, on a signalé que les nouvelles crises postopératoires étaient plus fréquentes chez les patients ayant subi une résection totale grossière (46). Une explication possible est qu’une manipulation, une dissection et une rétraction plus importantes du cerveau pour réaliser une résection totale grossière peuvent provoquer des lésions corticales, une irritation, un œdème et des crises. Dans une étude, la résection de grade I de Simpson était corrélée à des crises postopératoires (39). La plupart de ces lésions étaient des méningiomes à convexité, qui sont fortement corrélés avec les crises d’épilepsie. Par conséquent, le classement de Simpson n’était pas cliniquement pertinent dans cette étude. Des résultats similaires ont été rapportés par Hess et al, sans qu’aucune signification statistique ne soit notée entre le grade de Simpson et les crises postopératoires (35). De multiples études ont montré une association entre les crises et la récurrence/progression tumorale (23, 47). Une théorie postulée est qu’il y a une possible réactivation d’un foyer épileptogène antérieur ou la formation d’un nouveau foyer avec la récurrence de la tumeur (40, 43). Les lésions de grade I de l’OMS ont de faibles taux de récidive et, en cas de résection totale grossière, cela peut être un facteur de protection contre les crises postopératoires (4, 5).
Most of the literature data report an absence of crises after a craniotomy and resection, and few studies deal with other treatment methods such as radiosurgery. Kondziolka et al. reported a case of mortality without more details (54). In Zada's study on 116 patients who have undergone treatment by gamma knife for meningioma, there was no crisis over the 75 months of follow -up (55). Pollack et al. pointed out a rate of 1.6 % of new or aggravated crises after radiosurgery (56). A decrease in freedom of crisis was reported after surgery in patients with intractable crises in preoperative (40).
Unaccompanied epilepsy management linked to meningioma; Medicines and epilepsy surgery
L’Académie américaine de neurologie ne recommande pas l’utilisation prophylactique des ASM dans les cas de tumeurs cérébrales nouvellement diagnostiquées. Dans notre institution, nous ne préconisons pas l’obtention d’un EEG préopératoire pour aider à déterminer si le patient doit être placé sous ASM. Pourtant, certains chirurgiens préconisent l’utilisation prophylactique des ASM dans la période postopératoire immédiate afin de prévenir les crises dé-novo (57). Dans une étude de Zheng et al. les ASM ont réduit le risque de crises postopératoires précoces (8, 58). Les ASM peuvent être utilisés chez les patients présentant des crises préopératoires comme mesure temporaire jusqu’à la résection chirurgicale. On estime que 40 % des patients dont les crises étaient bien contrôlées avant l’intervention chirurgicale ont pu être sevrés des ASM au cours des 27 mois postopératoires, et que seuls 22 % sont restés avec des crises intraitables (8). Pour une meilleure sélection des patients et une meilleure utilisation des ASM en postopératoire, le système de notation STAMPE a été une tentative pour aider à guider le traitement de l’épilepsie chez les patients atteints de méningiome (19). Ils ont proposé un système de notation simple comprenant des facteurs de risque possibles tels que le déficit sensorimoteur, la progression de la tumeur, l’âge < 55 ans, une complication chirurgicale majeure, les crises préopératoires, l’EEG postopératoire et l’œdème cérébral. Les résultats n’étaient cependant pas statistiquement significatifs et nécessitaient une validation supplémentaire.
The evaluation of epilepsy surgery for further resection after having delimited the epileptogenic zone by intracranial EEG monitoring (grids, bands or stereotaxic electrodes), including peroperative ECOG, is the reference approach in level 4 epilepsy centers for patients with lesional epilepsy that did not respond to at least two ASM selected and dosed. The EEG can be useful to assess the recurrence of crises when weaning or stopping ASM. Several studies have suggested the systematic use of the POSE EEG to predict the recurrence of crises. In a study on 340 patients, the epileptiform discharge made it possible to predict postoperative crises, which pleads in favor of the systematic use of the EEG in postoperative (19). The peroperative mapping of ECOG and the resection of the secondary crisis home in the peritumoral cortex can increase the rates of absence of a postoperative crisis (23, 27). The postoperative EEG with epileptiform discharges is suggested as a predictor of the appearance of postoperative crises (19, 59). However, the American Academy of Neurology has published a practice directive in adult epileptic patients who obtained an absence of crisis (but not specifically for meningioma), the order of an EEG to detect inter -scileptive discharges is not useful to guide the decision to prosecute the ASM. However, this approach is more reliable in pediatric patients. An epileptiform potential on EEG in pediatric patients increases the risk of crisis recurrence (60).
In our center, we evaluate each patient with epilepsy linked to meningioma, in particular patients who continue to have uncontrolled postoperative seizures with the implementation of deep stereotaxic electrodes (S-EEG) or by under-dural/band underline electrodes, and in cases where functional cartography is essential to exclude the implication of the cortex epileptogenic. S-EEG is a safer option for patients who must undergo a second surgical intervention, knowing that the complications of the previous intervention, such as adhesions, infections, bleeding, etc. are likely to be a problem. Rise functional mapping can also be carried out by EEG-S in comparison with the detailed functional map carried out by grid or band electrodes. In areas where safer resection is possible outside the eloquent cortex, EEG-S is useful for encompassing the edges of the lesion and to reach distant areas of interest, such as mesial temporal structures, in order to exclude a double pathology.
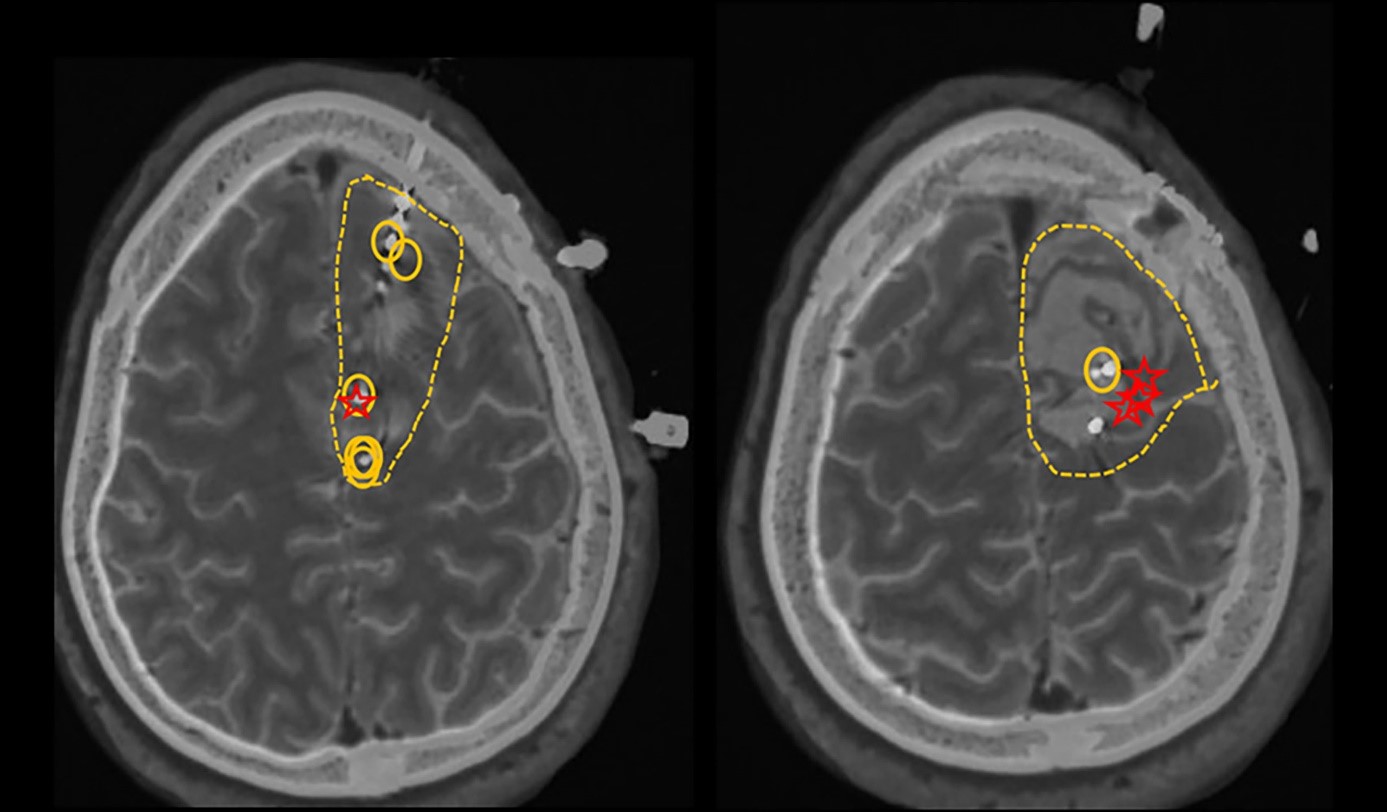
The following case illustrates our own experience in the management of postoperative crises after a resection of meningioma. A left -handed 36 -year -old man who underwent a median left -wing parasagittal meningiomal (6 x 7 cm) and has developed recent appearance seizures 8 to 10 months after the operation. His MRI 3 months after the operation showed a complete resection of the tumor. About 11 months after resection, he developed his first crisis "Tonico-Clonique". It started with numbness, weakness and tingling on the right side of his back, descending towards the middle of his spine. It was then put under lamotrigine, but continued to have repeated crises which began with the same feelings of swarming to the spine, associated with abnormal sensations of butterfly in the abdomen, to finally lead to movements of trembling of the right foot, with propagation to the right arm. Due to the development of drug-resistant epilepsy (ERD), including lamotrigine, lacosamide and Levetiracetam, he underwent additional surgical evaluation of epilepsy, including an EEG video of the scalp and intracranial EEG monitoring with stereotaxic intracranial S-EEG monitoring, which has better Epileptogenic zone in the central and paracentral frontal channels left behind the posterior and mesial margins of the surgical cavity, with probably an earlier appearance on the mesial surface on the left side of the interhemispherical crack given the early implication of the right foot (Figure 1). About 25 months after initial surgery, he underwent a second left frontal craniotomy programmed for the resection of epileptogenic foci. He continued to take anticonvulsant drugs after the operation and reported an improvement in the frequency of crises. Since he underwent his second surgery, there has been a significant reduction in the frequency of crises, which has gone from twice a week to twice a year, of the conscious focal type triggered by the reduction of drugs or the consumption of alcohol.
MRI 1
IRM 1 Les cercles représentent les décharges épileptiformes interictales actives (les zones irritatives). Les étoiles représentent les premiers contacts impliqués au début de l’épisode épileptique. Les lignes pointillées représentent la zone de résection proposée.
This case report is used as an example to show the complexity of the management of a patient with meningioma having undergone a craniotomy. A separate project approved by the IRB will be carried out to retrospectively analyze the success rate of such procedures in our center.
Regarding the medical treatment of primary brain tumors (TCP) in general, there are no solid and randomized studies to support the choice of ASMs. Several factors should be taken into account, including sex, age, cost, profession, cognition, common side effects of drugs, the neurological base linked to tumor/surgery (in order to avoid the addition of the undesirable effects of drugs), pharmacokinetics of drugs, drug interactions, efficiency and comorbidities. It is also necessary to take into account the interaction with chemotherapy treatments and the effect of radiation on the brain. Certain types of tumors (such as low-grade tumors) are known to be resistant to ASM treatment due to several hypotheses such as the intrinsic severity of the underlying mechanism of epileptogenicity, the altered expression of the molecules on which the ASM act or the modification of the expression of the transporters at the level of the hemato-encephalic barrier limiting the penetration of the drug epileptogenic (61). The most recent ASMs (oxcarbazepine, topiramate, lamotrigine, levetiracetam, zonisamide and lacosamide) have better tolerance and better efficiency due to different aspects, including their property of not indzyme, their limited interaction between drugs, their pure kidney excretion and their lesser side effects. Old generation ASMs such as carbamazepine, phenytoin and phenobarbital are falling into disuse because of their strong protein bond, drug interactions and the induction of the hepatic P-450. The undesirable effects of ASMs are reported as higher in PBT patients than in the general population of epileptics (24% vs 0.5-12%) (57). In PBTS, the undesirable effects of the ASMS directed towards the brain function such as the executive function, the attention of attention, the cognitive function are six times higher than the undesirable effects linked to the irradiation of the brain (62). Overall, the best risk-benefit report for the choice of ASM to be used is based on the doctor's judgment. It is very important to mention that treatment must be started after a single crisis. According to the recommendations of the American Academy of Neurology (ANA), it is not necessary to administer a prophylactic treatment by ASM to patients with brain tumors without a history of crises. It is also suggested that the gradual decrease and the stop of ASM after the first postoperative week are appropriate in the absence of crisis history (57). In summary, the strategy of selecting drugs for the management of the BTR must promote parenteral administration drugs, the ASMs which do not require slow titration, and must avoid enzymatic inductors. If monotherapy fails, you must consider combined therapy, poor compliance, repeated surgery and tumor recurrence/progression.
The efficiency of each ASM is very variable: oxcarbazepine in monotherapy: 62.9 %; Topiramate in monotherapy: 55.6 %; Gabapentine, pregabalin, tiagabine, zonisamide in extra treatment: 27.4 to 100 %; Levetiracetam in monotherapy and extra treatment: 47.4% at 88%; Lacosamide as an extra medication with 42.9% (63). Levetiracetam and valproic acid are the most studied drugs in epilepsy linked to tumors. Levétiracétam was studied compared to valproic acid and the failure of the treatment of crises in glioblastoma was 33% against 50%, perhaps because of its tolerance and its property to strengthen the inhibition of methylguanine-add Methyltransferase by P53 in this population of patients (64). The most attractive factors for the popularity of the Levetiracetam are its good tolerance, its ease of use without the need for titration, the lack of interaction with other ASM, its hepatic non-metabolization by the CYP450, and therefore the lack of interaction with certain chemotherapy drugs used in certain cases of BTR, and finally good insurance coverage.
In a recent survey published on ASM preferences of prescriptions among European neuro-oncologists, Levetiracetam is considered to be the first choice for patients with brain tumors, with the highest presumed efficiency and the weakest adverse effects (65). ASMs differ by their pharmacokinetics, their therapeutic efficiency and their side effects, which were examined in detail by Maschio (63).
La prise en charge des crises doit aller au-delà des options pharmacologiques. Les crises non traitées peuvent exposer les patients à un risque d’issue catastrophique, comme la mort subite inattendue chez les patients épileptiques. En outre, les crises peuvent avoir un impact négatif sur le mode de vie des patients, notamment sur le travail, l’emploi, l’éducation et la conduite automobile. Le risque de blessure physique ou de décès n’est pas limité au conducteur et aux passagers, mais s’applique aux piétons et aux personnes se trouvant dans d’autres véhicules. Les différents États américains ont des lois différentes pour déterminer quel groupe de patients épileptiques peut conduire. Les crises peuvent entraîner d’autres blessures physiques. Les patients souffrant d’épilepsie réfractaire doivent être traités dans des centres tertiaires où ils peuvent bénéficier d’un soutien médical, social et comportemental et, surtout, d’une évaluation en vue d’une chirurgie épileptique.
Future prospects
Malgré les progrès réalisés dans la compréhension des mécanismes physiopathologiques et la prise en charge de l’épilepsie liée aux méningiomes, d’importantes lacunes dans les connaissances subsistent.
Parmi les questions pertinentes, citons : » quels sont les patients les plus exposés au risque de crises épileptiques ? » et » quand commencer les ASM et pendant combien de temps ? « .
The risk of persistent postoperative crises highlights the need to continue research on crises in patients with meningioma. The arbitrary and long -term use of ASMs in patients with meningioma highlights the importance of directives for appropriate selection of patients. Thus, randomized prospective trials are necessary to guide the selection and prescription of ASMs. Stop 'EM is a controlled randomized trial in progress, the end date of which is set at September 2027 (66). It aims to determine the need to use postoperative ASM in patients who have never had an epileptic crisis. The main objectives of the study are to determine the effectiveness of the levetiracetam in crisis prevention over a period of 12 months after surgery, the effect of starting the levetiracetam on the ability to resume conduct, quality of life and cost-effectiveness.
Conclusion
Comprendre et prédire les crises d’épilepsie liées à un méningiome peut aider à guider le contrôle des crises et permettre de mieux déterminer les patients à risque avant et après la chirurgie. La littérature médicale actuelle fournit des données limitées pour la prédiction des crises postopératoires et la gestion optimale des patients atteints d’épilepsie liée à un méningiome.
With regard to the cohort of patients with meningioma and undergoing surgery, stratified according to the state of preoperative crisis compared to the postoperative crisis state, it is logical to identify four different groups:
- without crisis in relation to the state of crisis,
- with crisis in relation to the state of crisis,
- without crisis in relation to the state of crisis
- And with crisis in relation to the state of crisis.
Les efforts futurs de stratification des patients dans ces quatre groupes, y compris les médicaments seuls, la chirurgie/les interventions seules, les médicaments + la chirurgie/les interventions, permettront de prédire le résultat de l’intervention chirurgicale et de traiter les patients de manière optimale avec les modalités les plus efficaces.
Contributions from authors
Re, HT, LH, WB and FB contributed to the design and design of the study. RE wrote the first version of the manuscript. AA has written sections of the manuscript. HT, LH, AA, WB and FB contributed to the revision of the manuscript. All the authors approved the submissive version.
Conflict of interest
The authors declare that research has been carried out in the absence of any commercial or financial relationship which could be interpreted as a potential conflict of interest.
Publisher's note
All the claims expressed in this article only engage the authors and do not necessarily represent those of their affiliated organizations, nor those of the publisher, editors and revisers. Any product evaluated in this article, or any claim made by its manufacturer, is neither guaranteed nor approved by the publisher.
Thanks
This study was supported by the subsidy (n ° 19140900105) of the Shanghai Science and Technology Committee and by the Research Fund of the Neurosurgery Department of the University of Loma Linda.
References
- Wiemels J, Wrensch M, Claus EB. Epidemiology and Etiology of Meningioma. J Neurooncol (2010) 99(3):307–14. doi: 10.1007/s11060-010-0386-3
Pubmed abstract | Crossref Full Text | Google Scholar
- Porter KR, McCarthy BJ, Freels S, Kim Y, Davis FG. Prevalence Estimates for Primary Brain Tumors in the United States by Age, Gender, Behavior, and Histology. Neuro Oncol (2010) 12(6):520–7. doi: 10.1093/neuonc/nop066
Pubmed abstract | Crossref Full Text | Google Scholar
- Ostrom QT, Gittleman H, Fulop J, Liu M, Blanda R, Kromer C, et al. CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2008-2012. Neuro Oncol (2015) 17 Suppl 4:iv1–iv62. doi: 10.1093/neuonc/nov189
Pubmed abstract | Crossref Full Text | Google Scholar
- Sughrue ME, Kane AJ, Shangari G, Rutkowski MJ, McDermott MW, Berger MS, et al. The Relevance of Simpson Grade I and II Resection in Modern Neurosurgical Treatment of World Health Organization Grade I Meningiomas. J Neurosurg (2010) 113(5):1029–35. doi: 10.3171/2010.3.JNS091971
Pubmed abstract | Crossref Full Text | Google Scholar
- Hasseleid BF, Meling TR, Ronning P, Scheie D, Helseth E. Surgery for Convexity Meningioma: Simpson Grade I Resection as the Goal: Clinical Article. J Neurosurg (2012) 117(6):999–1006. doi: 10.3171/2012.9.JNS12294
Pubmed abstract | Crossref Full Text | Google Scholar
- Erturk Cetin O, Isler C, Uzan M, Ozkara C. Epilepsy-Related Brain Tumors. Seizure (2017) 44:93–7. doi: 10.1016/j.seizure.2016.12.012
Pubmed abstract | Crossref Full Text | Google Scholar
- Englot DJ, Magill ST, Han SJ, Chang EF, Berger MS, McDermott MW. Seizures in Supratentorial Meningioma: A Systematic Review and Meta-Analysis. J Neurosurg (2016) 124(6):1552–61. doi: 10.3171/2015.4.JNS142742
Pubmed abstract | Crossref Full Text | Google Scholar
- Chaichana KL, Pendleton C, Zaidi H, Olivi A, Weingart JD, Gallia GL, et al. Seizure Control for Patients Undergoing Meningioma Surgery. World Neurosurg (2013) 79(3-4):515–24. doi: 10.1016/j.wneu.2012.02.051
Pubmed abstract | Crossref Full Text | Google Scholar
- Van Breemen MS, Wilms EB, Vecht CJ. Seizure Control in Brain Tumors. Handb Clin Neurol (2012) 104:381–9. doi: 10.1016/B978-0-444-52138-5.00026-8
Pubmed abstract | Crossref Full Text | Google Scholar
- Bauer R, Ortler M, Seiz-Rosenhagen M, Maier R, Anton JV, Unterberger I. Treatment of Epileptic Seizures in Brain Tumors: A Critical Review. Neurosurg Rev (2014) 37(3):381–8:discussion 8. doi: 10.1007/s10143-014-0538-6
Pubmed abstract | Crossref Full Text | Google Scholar
- Taphoorn MJ, Klein M. Cognitive Deficits in Adult Patients With Brain Tumours. Lancet Neurol (2004) 3(3):159–68. doi: 10.1016/S1474-4422(04)00680-5
Pubmed abstract | Crossref Full Text | Google Scholar
- Gilliam F, Kuzniecky R, Faught E, Black L, Carpenter G, Schrodt R. Patient-Validated Content of Epilepsy-Specific Quality-of-Life Measurement. Epilepsia (1997) 38(2):233–6. doi: 10.1111/j.1528-1157.1997.tb01102.x
Pubmed abstract | Crossref Full Text | Google Scholar
- Chaichana KL, Parker SL, Olivi A, Quinones-Hinojosa A. Long-Term Seizure Outcomes in Adult Patients Undergoing Primary Resection of Malignant Brain Astrocytomas. Clinical Article. J Neurosurg (2009) 111(2):282–92. doi: 10.3171/2009.2.JNS081132
Pubmed abstract | Crossref Full Text | Google Scholar
- Harden CL. The Co-Morbidity of Depression and Epilepsy: Epidemiology, Etiology, and Treatment. Neurology (2002) 59(6 Suppl 4):S48–55. doi: 10.1212/WNL.59.6_suppl_4.S48
Pubmed abstract | Crossref Full Text | Google Scholar
- Cramer JA, Mintzer S, Wheless J, Mattson RH. Adverse Effects of Antiepileptic Drugs: A Brief Overview of Important Issues. Expert Rev Neurother (2010) 10(6):885–91. doi: 10.1586/ern.10.71
Pubmed abstract | Crossref Full Text | Google Scholar
- Hamasaki T, Yamada K, Kuratsu J. Seizures as a Presenting Symptom in Neurosurgical Patients: A Retrospective Single-Institution Analysis. Clin Neurol Neurosurg (2013) 115(11):2336–40. doi: 10.1016/j.clineuro.2013.08.016
Pubmed abstract | Crossref Full Text | Google Scholar
- Seyedi JF, Pedersen CB, Poulsen FR. Risk of Seizures Before and After Neurosurgical Treatment of Intracranial Meningiomas. Clin Neurol Neurosurg (2018) 165:60–6. doi: 10.1016/j.clineuro.2018.01.002
Pubmed abstract | Crossref Full Text | Google Scholar
- Chozick BS, Reinert SE, Greenblatt SH. Incidence of Seizures After Surgery for Supratentorial Meningiomas: A Modern Analysis. J Neurosurg (1996) 84(3):382–6. doi: 10.3171/jns.1996.84.3.0382
Pubmed abstract | Crossref Full Text | Google Scholar
- Wirsching HG, Morel C, Gmur C, Neidert MC, Baumann CR, Valavanis A, et al. Predicting Outcome of Epilepsy After Meningioma Resection. Neuro Oncol (2016) 18(7):1002–10. doi: 10.1093/neuonc/nov303
Pubmed abstract | Crossref Full Text | Google Scholar
- Chen WC, Magill ST, Englot DJ, Baal JD, Wagle S, Rick JW, et al. Factors Associated With Pre- and Postoperative Seizures in 1033 Patients Undergoing Supratentorial Meningioma Resection. Neurosurgery (2017) 81(2):297–306. doi: 10.1093/neuros/nyx001
Pubmed abstract | Crossref Full Text | Google Scholar
- Lieu AS, Howng SL. Intracranial Meningiomas and Epilepsy: Incidence, Prognosis and Influencing Factors. Epilepsy Res (2000) 38(1):45–52. doi: 10.1016/S0920-1211(99)00066-2
Pubmed abstract | Crossref Full Text | Google Scholar
- Morsy MM, El-Saadany WF, Moussa WM, Sultan AE. Predictive Factors for Seizures Accompanying Intracranial Meningiomas. Asian J Neurosurg (2019) 14(2):403–9. doi: 10.4103/ajns.AJNS_152_18
Pubmed abstract | Crossref Full Text | Google Scholar
- Xue H, Sveinsson O, Bartek J Jr., Forander P, Skyrman S, Kihlstrom L, et al. Long-Term Control and Predictors of Seizures in Intracranial Meningioma Surgery: A Population-Based Study. Acta Neurochir (Wien) (2018) 160(3):589–96. doi: 10.1007/s00701-017-3434-3
Pubmed abstract | Crossref Full Text | Google Scholar
- Schaller B. Brain Tumor and Seizures: Pathophysiology and its implications for Treatment Revisited (Epilepsia 2003; 44: 1223-1232). Epilepsia (2006) 47 (3): 661; discussion. DOI: 10.1111/J.1528-1167.2006.00484_1.x
Crossref Full Text | Google Scholar
- Gadot R, Khan AB, Patel R, Goethe E, Shetty A, Hadley CC, et al. Predictors of Postoperative Seizure Outcome in Supratentorial Meningioma. J Neurosurg (2021), 1–10. doi: 10.3171/2021.9.JNS211738
Pubmed abstract | Crossref Full Text | Google Scholar
- Shamji MF, Fric-Shamji EC, Benoit BG. Brain Tumors and Epilepsy: Pathophysiology of Peritumoral Changes. Neurosurg Rev (2009) 32(3):275–84; discussion 84-6. doi: 10.1007/s10143-009-0191-7
Pubmed abstract | Crossref Full Text | Google Scholar
- Fang S, Zhan Y, Xie YF, Shi Q, Dan W. Predictive Value of Electrocorticography for Postoperative Epilepsy in Patients With Supratentorial Meningioma. J Clin Neurosci (2013) 20(1):112–6. doi: 10.1016/j.jocn.2012.02.021
Pubmed abstract | Crossref Full Text | Google Scholar
- van Diessen E, Diederen SJ, Braun KP, Jansen FE, Stam CJ. Functional and Structural Brain Networks in Epilepsy: What Have We Learned? Epilepsia (2013) 54(11):1855–65. doi: 10.1111/epi.12350
Pubmed abstract | Crossref Full Text | Google Scholar
- Mehta N, Bhagwati S, Parulekar G. Meningiomas in Children: A Study of 18 Cases. J Pediatr Neurosci (2009) 4(2):61–5. doi: 10.4103/1817-1745.57322
Pubmed abstract | Crossref Full Text | Google Scholar
- Simis A, Pires de Aguiar PH, Leite CC, Santana PA Jr., Rosemberg S, Teixeira MJ. Peritumoral Brain Edema in Benign Meningiomas: Correlation With Clinical, Radiologic, and Surgical Factors and Possible Role on Recurrence. Surg Neurol (2008) 70(5):471–7; discussion 7. doi: 10.1016/j.surneu.2008.03.006
Pubmed abstract | Crossref Full Text | Google Scholar
- Lobato RD, Alday R, Gomez PA, Rivas JJ, Dominguez J, Cabrera A, et al. Brain Oedema in Patients With Intracranial Meningioma. Correlation Between Clinical, Radiological, and Histological Factors and the Presence and Intensity of Oedema. Acta Neurochir (Wien) (1996) 138(5):485–93; discussion 93-4. doi: 10.1007/BF01411166
Pubmed abstract | Crossref Full Text | Google Scholar
- Kawaguchi T, Kameyama S, Tanaka R. Peritumoral Edema and Seizure in Patients With Cerebral Convexity and Parasagittal Meningiomas. Neurol Med Chir (Tokyo) (1996) 36(8):568–73; discussion 73-4. doi: 10.2176/nmc.36.568
Pubmed abstract | Crossref Full Text | Google Scholar
- Yoshioka H, Hama S, Taniguchi E, Sugiyama K, Arita K, Kurisu K. Peritumoral Brain Edema Associated With Meningioma: Influence of Vascular Endothelial Growth Factor Expression and Vascular Blood Supply. Cancer (1999) 85(4):936–44. doi: 10.1002/(sici)1097-0142(19990215)85:4
Pubmed abstract | Crossref Full Text | Google Scholar
- Pistolesi S, Fontanini G, Camacci T, De Ieso K, Boldrini L, Lupi G, et al. Meningioma-Associated Brain Oedema: The Role of Angiogenic Factors and Pial Blood Supply. J Neurooncol (2002) 60(2):159–64. doi: 10.1023/a:1020624119944
Pubmed abstract | Crossref Full Text | Google Scholar
- Hess K, Spille DC, Adeli A, Sporns PB, Brokinkel C, Grauer O, et al. Brain Invasion and the Risk of Seizures in Patients With Meningioma. J Neurosurg (2018) 130(3):789–96. doi: 10.3171/2017.11.JNS172265
Pubmed abstract | Crossref Full Text | Google Scholar
- de Vries J, Wakhloo AK. Cerebral Oedema Associated With WHO-I, WHO-II, and WHO-III-Meningiomas: Correlation of Clinical, Computed Tomographic, Operative and Histological Findings. Acta Neurochir (Wien) (1993) 125(1-4):34–40. doi: 10.1007/BF01401825
Pubmed abstract | Crossref Full Text | Google Scholar
- Chernov MF, Kasuya H, Nakaya K, Kato K, Ono Y, Yoshida S, et al. (1)H-MRS of Intracranial Meningiomas: What it can Add to Known Clinical and MRI Predictors of the Histopathological and Biological Characteristics of the Tumor? Clin Neurol Neurosurg (2011) 113(3):202–12. doi: 10.1016/j.clineuro.2010.11.008
Pubmed abstract | Crossref Full Text | Google Scholar
- Spille DC, Hess K, Sauerland C, Sanai N, Stummer W, Paulus W, et al. Brain Invasion in Meningiomas: Incidence and Correlations With Clinical Variables and Prognosis. World Neurosurg (2016) 93:346–54. doi: 10.1016/j.wneu.2016.06.055
Pubmed abstract | Crossref Full Text | Google Scholar
- Islim AI, McKeever S, Kusu-Orkar TE, Jenkinson MD. The Role of Prophylactic Antiepileptic Drugs for Seizure Prophylaxis in Meningioma Surgery: A Systematic Review. J Clin Neurosci (2017) 43:47–53. doi: 10.1016/j.jocn.2017.05.020
Pubmed abstract | Crossref Full Text | Google Scholar
- Lu VM, Wahood W, Akinduro OO, Parney IF, Quinones-Hinojosa A, Chaichana KL. Four Independent Predictors of Postoperative Seizures After Meningioma Surgery: A Meta-Analysis. World Neurosurg (2019) 130:537–45 e3. doi: 10.1016/j.wneu.2019.06.063
Pubmed abstract | Crossref Full Text | Google Scholar
- Wilson Ta, Huang L, Ramanathan D, Lopez-Gonzalez M, Pillai P, de los Reyes K, et al. Review of Atypical and Anaplastic Meningiomas: Classification, Molecular Biology, and Management. Front Oncol (2020) 10: 565582. DOI: 10.3389/FONC. 2010.565582
Pubmed abstract | Crossref Full Text | Google Scholar
- Tsuji M, Shinomiya S, Inoue R, Sato K. Prospective Study of Postoperative Seizure in Intracranial Meningioma. Jpn J Psychiatry Neurol (1993) 47(2):331–4. doi: 10.1111/j.1440-1819.1993.tb02094.x
Pubmed abstract | Crossref Full Text | Google Scholar
- Li X, Wang C, Lin Z, Zhao M, Ren X, Zhang X, et al. Risk Factors and Control of Seizures in 778 Chinese Patients Undergoing Initial Resection of Supratentorial Meningiomas. Neurosurg Rev (2020) 43(2):597–608. doi: 10.1007/s10143-019-01085-5
Pubmed abstract | Crossref Full Text | Google Scholar
- Hamasaki T, Yamada K, Yano S, Nakamura H, Makino K, Hide T, et al. Higher Incidence of Epilepsy in Meningiomas Located on the Premotor Cortex: A Voxel-Wise Statistical Analysis. Acta Neurochir (Wien) (2012) 154(12):2241–9. doi: 10.1007/s00701-012-1511-1
Pubmed abstract | Crossref Full Text | Google Scholar
- McGovern SL, Aldape KD, Munsell MF, Mahajan A, DeMonte F, Woo SY. A Comparison of World Health Organization Tumor Grades at Recurrence in Patients With non-Skull Base and Skull Base Meningiomas. J Neurosurg (2010) 112(5):925–33. doi: 10.3171/2009.9.JNS09617
Pubmed abstract | Crossref Full Text | Google Scholar
- Baumgarten P, Sarlak M, Baumgarten G, Marquardt G, Seifert V, Strzelczyk A, et al. Focused Review on Seizures Caused by Meningiomas. Epilepsy Behav (2018) 88:146–51. doi: 10.1016/j.yebeh.2018.09.002
Pubmed abstract | Crossref Full Text | Google Scholar
- Zheng Z, Chen P, Fu W, Zhu J, Zhang H, Shi J, et al. Early and Late Postoperative Seizure Outcome in 97 Patients With Supratentorial Meningioma and Preoperative Seizures: A Retrospective Study. J Neurooncol (2013) 114(1):101–9. doi: 10.1007/s11060-013-1156-9
Pubmed abstract | Crossref Full Text | Google Scholar
- Beghi E, Carpio A, Forsgren L, Hesdorffer DC, Malmgren K, Sander JW, et al. Recommendation for a Definition of Acute Symptomatic Seizure. Epilepsia (2010) 51(4):671–5. doi: 10.1111/j.1528-1167.2009.02285.x
Pubmed abstract | Crossref Full Text | Google Scholar
- Baumgarten P, Sarlak M, Monden D, Spyrantis A, Bernatz S, Gessler F, et al. Early and postoperative late seizures in meningioma patients and prediction by a recent scoring system. Cancers (Basel) (2021) 13 (3): 450. DOI: 10.3390/Cancers13030450
Pubmed abstract | Crossref Full Text | Google Scholar
- Joiner EF, Youngerman BE, Hudson TS, Yang J, Welch MR, McKhann GM, et al. Effectiveness of Perioperative Antiepileptic Drug Prophylaxis for Early and Late Seizures Following Oncologic Neurosurgery: A Meta-Analysis. J Neurosurg (2018) 130(4):1–9. doi: 10.3171/2017.10.JNS172236
Pubmed abstract | Crossref Full Text | Google Scholar
- Raza SM, Gallia GL, Brem H, Weingart JD, Long DM, Olivi A. Perioperative and Long-Term Outcomes From the Management of Parasagittal Meningiomas Invading the Superior Sagittal Sinus. Neurosurgery (2010) 67(4):885–93; discussion 93. doi: 10.1227/NEU.0b013e3181ef2a18
Pubmed abstract | Crossref Full Text | Google Scholar
- Scott DF. Left and Right Cerebral Hemisphere Differences in the Occurrence of Epilepsy. Br J Med Psychol (1985) 58( Pt 2):189–92. doi: 10.1111/j.2044-8341.1985.tb02633.x
Pubmed abstract | Crossref Full Text | Google Scholar
- Islim AI, Ali A, Bagchi A, Ahmad MU, Mills SJ, Chavredakis E, et al. Postoperative Seizures in Meningioma Patients: Improving Patient Selection for Antiepileptic Drug Therapy. J Neurooncol (2018) 140(1):123–34. doi: 10.1007/s11060-018-2941-2
Pubmed abstract | Crossref Full Text | Google Scholar
- Komotar RJ, Raper DM, Starke RM, Iorgulescu JB, Gutin PH. Prophylactic Antiepileptic Drug Therapy in Patients Undergoing Supratentorial Meningioma Resection: A Systematic Analysis of Efficacy. J Neurosurg (2011) 115(3):483–90. doi: 10.3171/2011.4.JNS101585
Pubmed abstract | Crossref Full Text | Google Scholar
- Zada G, Pagnini PG, Yu C, Erickson KT, Hirschbein J, Zelman V, et al. Long-Term Outcomes and Patterns of Tumor Progression After Gamma Knife Radiosurgery for Benign Meningiomas. Neurosurgery (2010) 67(2):322–8; discussion 8-9. doi: 10.1227/01.NEU.0000371974.88873.15
Pubmed abstract | Crossref Full Text | Google Scholar
- Pollock BE, Stafford SL, Link MJ, Garces YI, Foote RL. Single-Fraction Radiosurgery for Presumed Intracranial Meningiomas: Efficacy and Complications From a 22-Year Experience. Int J Radiat Oncol Biol Phys (2012) 83(5):1414–8. doi: 10.1016/j.ijrobp.2011.10.033
Pubmed abstract | Crossref Full Text | Google Scholar
- Glantz MJ, Cole BF, Forsyth PA, Recht LD, Wen PY, Chamberlain MC, et al. Practice Parameter: Anticonvulsant Prophylaxis in Patients With Newly Diagnosed Brain Tumors. Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology (2000) 54(10):1886–93. doi: 10.1212/WNL.54.10.1886
Pubmed abstract | Crossref Full Text | Google Scholar
- Zhang B, Zhao G, Yang HF, Wang D, Yu JL, Huang HY. Assessment of Risk Factors for Early Seizures Following Surgery for Meningiomas Using Logistic Regression Analysis. J Int Med Res (2011) 39(5):1728–35. doi: 10.1177/147323001103900515
Pubmed abstract | Crossref Full Text | Google Scholar
- Harward SC, Rolston JD, Englot DJ. Seizures in Meningioma. Handb Clin Neurol (2020) 170:187–200. doi: 10.1016/B978-0-12-822198-3.00053-7
Pubmed abstract | Crossref Full Text | Google Scholar
- Gloss D, Pargeon K, Pack A, Varma J, French JA, Tolchin B, et al. Antiseizure Medication Withdrawal in Seizure-Free Patients: Practice Advisory Update Summary: Report of the AAN Guideline Subcommittee. Neurology (2021) 97(23):1072–81. doi: 10.1212/WNL.0000000000012944
Pubmed abstract | Crossref Full Text | Google Scholar
- Guerrini R, Rosati A, Giordano F, Genitori L, Barba C. The Medical and Surgical Treatment of Tumoral Seizures: Current and Future Perspectives. Epilepsia (2013) 54:84–90. doi: 10.1111/epi.12450
Pubmed abstract | Crossref Full Text | Google Scholar
- Klein M. Neurocognitive Functioning in Adult WHO Grade II Gliomas: Impact of Old and New Treatment Modalities. Neuro Oncol (2012) 14:17–24. doi: 10.1093/neuonc/nos161
Crossref Full Text | Google Scholar
- Maschio M, Dinapoli L, Sperati F, Pace A, Fabi A, Vidiri A, et al. Effect of Pregabalin Add-on Treatment on Seizure Control, Quality of Life, and Anxiety in Patients With Brain Tumour-Related Epilepsy: A Pilot Study. Epileptic Disord (2012) 14(4):388–97. doi: 10.1684/epd.2012.0542
Pubmed abstract | Crossref Full Text | Google Scholar
- van der Meer PB, Dirven L, Fiocco M, Vos MJ, Kouwenhoven MCM, van den Bent MJ, et al. First-Line Antiepileptic Drug Treatment in Glioma Patients With Epilepsy: Levetiracetam vs Valproic Acid. Epilepsia (2021) 62(5):1119–29. doi: 10.1111/epi.16880
Pubmed abstract | Crossref Full Text | Google Scholar
- van der Meer PB, Dirven L, van den Bent MJ, Preusser M, Taphoorn MJB, Rudá R, et al. Prescription Preferences of Antiepileptic Drugs in Brain Tumor Patients: An International Survey Among EANO Members. Neuro-Oncol Pract (2021) 9(2):105–13. doi: 10.1093/nop/npab059
Crossref Full Text | Google Scholar
- Jenkinson M, Helmy A, Huckey H, Mills S, Grant R, Hughes D, et al. Surgeons Trial Of Prophylaxis For Epilepsy In Seizure Naïve Patients With Meningioma: A Randomized Controlled Trial (STOP ‘Em). Neuro-Oncol Pract (2020) 22(Supplement_2):ii195. doi: 10.1093/neuonc/noaa215.815
Crossref Full Text | Google Scholar