On December 18, 2024, the EPI-Phare scientific interest group presented to the temporary scientific committee (CST) “Oral contraception and Méningioma risk” of the ANSM, the results of its latest study on the risk of meningiom in women exposed to a progestogen in oral contraception. The study does not show an over-risk of meningioma for women using contraception containing levonorgestrel alone or combined with ethinylestradiol. It highlights a very low increase in the risk for deogestrel -based contraceptions during prolonged use in women over 45. Given these results, and pending the upcoming measures in early 2025, we issue preliminary recommendations for the use of these oral contraceptives and monitoring of women exposed to it.
The study carried out by EPI-PHARE (CNAM-ANSM scientific interest group), presented at the CST, is in line with previous work which has demonstrated a risk of meningiomas associated with certain progestins: Androcur (cyproterone acetate), Lutéran (chlormadinone acetate), Lutényl (nomegestrol), Dépo Provéra (medroxyprogesterone acetate), Colprone (medrogestone) and Sugestone (promegestone).
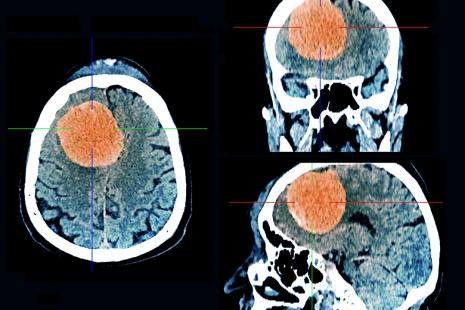
The study presented evaluates in real life the risk of intracranial meningiomal operated between 2020 and 2023 associated with the use of other contraceptive progestins: deogestrel (75µg), levonorgestrel (30µg) and the combination of levonorgestrel-ethinylestradiol (50-150µg). The potential risk of meningioma had not been evaluated before with the specific use of these oral contraceptives which are widely used in France.
This case-control study is based on data from the National Health Data System (SNDS). A total of 8,391 women operated with intracranial meningioma between 2020 and 2023 in France were included in the study.
The main results indicate that the use of Lévonorgestrel, alone or combined with ethinylestradiol, is not associated with an increase in the risk of intracranial meningioma, whatever the exposure durations.
On the other hand, a very low increase in the risk of meningioma has been identified in women over 45, during prolonged use and during contraceptives based on deogestrel alone dosed at 75µg. This risk increases with the duration of use: it appears from 5 years of use and is multiplied by 2 beyond 7 years of exposure. The risk of meningioma during the prolonged taking of the deogestrel is however much lower than that observed with the capture of Androcur (Cyproterone acetate), Lotéran (Chlormadinone acetate) and Lutényl (Nomestrol).
No risk of meningioma has been observed in the event of the use of less than one year of the deogestrel, except when using other risk progestins.
Overall, the study estimates that on average, an intracranial meningiomal case operated is observed for 67,000 women exposed to deogestrel regardless of the duration of exposure and a case for 17,000 women exposed more than 5 years.
In view of these results, CST experts gathered by the ANSM discussed measures to reduce the risk of meningioma linked to the use of deogestrel. Pending measures to reduce the risk to come in early 2025, we issue preliminary recommendations.
There is a very low increase in the risk of meningioma associated with the prolonged taking of these contraceptives for women over 45.
- Do not stop your contraception without the advice of a health professional because there is an unwanted risk of pregnancy.
- If you have frequent headaches, vision disorders, weakness in the arms or legs, paralysis, language or hearing disorders, smell disorders, convulsions, memory disorders, dizziness, consult your doctor, gynecologist or midwife. An MRI can be offered as a precautionary measure.
- In the event of a meningioma discovery, the treatment must be stopped in consultation with your doctor or midwife. A neurosurgical opinion is also required.
The following recommendations also apply:
- In the event of a history of meningioma or existing meningioma, progestin contraception or progestin treatment should no longer be used.
- Inform your doctor, a midwife of taking progestin treatments in the past.
- Contraception can evolve throughout your life and must be adapted to your needs and your state of health. It is therefore important to reassess with your prescriber the interest of the prosecution or the modification of your contraception every year until the age of menopause.
- We recall that after menopause, contraception should no longer be prescribed. Disogestrel is not a hormonal treatment of menopause.
If one of your patients under Désogestrel has evocative signs of meningiomas, we recommend making him perform an MRI of control
In the event of discovery of meningioma in a patient under deogestrel, stop treatment and systematically guide to a neurosurgeon. In the event of a history of meningioma or existing meningioma, progestin contraception or progestin treatment should no longer be used.
Before any prescription or change of progestin contraception, we recommend checking the previous treatments by progestins used by your patient and their duration of use. It will be necessary to assess with the patient the most suitable contraception to her situation with regard to this information.
In a woman, contraception must be reviewed annually with regard to her age, her lifestyle and her history.
Disogestrel has a MA in contraception only and should not be used as a hormonal treatment of menopause.
As France Assos Santé writes, we believe that while this new study sheds some light on the issue, thepicture of meningioma risks associated with progestins is not yet complete. Indeed, between 2009 and 2018, the progestin Visanne and its generics, whose active ingredient is dienogest, were not prescribed frequently enough to generate reliable statistical data allowing conclusions to be drawn about its safety. However, its prescription has increased significantly since 2020, particularly for treating endometriosis.
The need for direct information
France Asso santé believes that all mechanisms must be activated to inform the people concerned as quickly and directly as possible, in accordance with the 2022 Patients' Rights Act, which specifies that "when, after the execution of investigations, treatments or preventive actions, new risks are identified, the person concerned must be informed, except in cases where it is impossible to find them".