Risk of intracranial meningiomal with three powerful progestins: a case-to-test study based on the population
Risk of intracranial meningioma with three powerful progestins
Current title: progestins and risk of meningioma
Léa Hoisnard1, Moussa Laanani1, Thibault Passi2, Lise Duranteau, Joël Coste4, Mahmoud
Zureik1, Sébastien Froelich2, and Alain Weill1
Affiliations of authors:
1 Scientific interest group of epidemiology of Epi-Phare health products, National Agency for the Safety of Medicines and Health Products, French Health Insurance, 93200 Saint-Denis, France
2 Department of Neurosurgery, Lariboisière Hospital, AP-HP, University of Paris, 75010 Paris, France
3 Medical gynecology service, Bicêtre Hospital, AP-HP, Paris Saclay University, 94270 Le Kremlin-Bicêtre, France
4 unit of biostatis and epidemiology-Cochin hospital, AP-HP, 75010 Paris, France
Correspondence to: Léa Hoisnard Scientific Interest Group Epi-Phare, 42 bd de la Liberation, 93200 Saint-Denis, France lea.hsnrd@gmail.com
This article was accepted for publication and was the subject of a complete peer examination, but was not subject to the processes of revision, composition, layout and correction of tests, which can lead to differences between this version and the official version. Please quote this article as DOI: 10.1111/ENE.15423
Context
A dose-dependent association between the use of cyproterone (Androcur) acetate and intracranial meningioma has been identified but the data concerning other progestins are rare. We evaluated the association between intracranial meningiomal surgery and exposure to three progestins: cyproterone acetate (CPA; ≥25 mg/day), nomestrol acetate (nomac; 3.75-5 mg/day) and chlormaudinone acetate (CMA; 2-10 mg/day).
Method
Dans cette étude cas-témoins basée sur la population nationale, les cas ont subi une chirurgie pour un méningiome intracrânien en France de 2009 à 2018. Ils ont été appariés à cinq témoins sur le sexe, l’année de naissance et la région de résidence. L’exposition aux progestatifs a été définie comme l’utilisation de progestatifs dans l’année précédant la chirurgie pour les cas ou à la même date pour leurs témoins.
Results
A total of 25,216 cases were included (75 % women, median age 58 years old).
Une exposition aux progestatifs a été notée pour 9,9 % des cas (2 497/25 216) et 1,9 % (2 382/126 080) des témoins, avec un odds ratio de 6,7 [IC 95 %, 6,3-7,1]. L’odds ratio était de 1,2 [1,0-1,4] pour une utilisation à court terme (< un an) et de 9,5 [8,8-10,2] pour une utilisation prolongée. Une forte association a été identifiée pour l’utilisation prolongée de CPA (OR=22,7 [19,5-26,4]), du NOMAC (OR=6,5 [5,8-7,2]) et du CMA (OR=4,7 [4,5-5,3]).
L’exposition aux progestatifs a augmenté le risque de méningiome pour tous les grades histologiques et tous les sites anatomiques, en particulier pour la base antérieure et moyenne du crâne : OR= 35,7 [26,5-48,2] et 23,9 [17,8-32,2] pour le CPA. Le nombre estimé de cas attribuables était de 2 124 [2028-2220] (212/an).
Conclusion
Nous avons observé une forte association entre l’exposition prolongée à des progestatifs puissants et la chirurgie pour méningiome. Le risque a augmenté de la chlormadinone au nomégestrol et à l’acétate de cyprotérone. Les individus doivent être informés de ce risque.
Mots clés : progestatifs, méningiome, acétate de cyprotérone, acétate de nomégestrol, acétate de chlormadinone
Introduction
Meningiomas are the most frequent intracranial tumors, representing 39 % of primitive tumors of the central nervous system1.
Les principaux facteurs de risque de méningiome sont l’âge, le fait d’être une femme, l’exposition aux rayonnements ionisants et la neurofibromatose de type 2 (NF2)2. Un certain nombre d’observations ont longtemps suggéré une association entre les hormones sexuelles endogènes et les méningiomes, sur la base de données épidémiologiques et d’études histopathologiques : il existe une incidence plus élevée chez les femmes (rapport 2,5/1), en particulier en âge de procréer1 ; des rapports de cas ont suggéré que la taille des méningiomes augmente pendant la grossesse et diminue après l’accouchement3,4 ; et des études biologiques ont montré que l’expression du récepteur de la progestérone pouvait être impliquée dans la survenue de certains types de méningiomes5-8.
Aucune association n’a été identifiée pour les contraceptifs oraux, pour lesquels les doses de progestatifs sont faibles. En ce qui concerne le traitement hormonal substitutif (THS) des femmes ménopausées, un certain nombre d’études épidémiologiques semblent soutenir un risque légèrement accru de méningiome mais les preuves sont limitées9,10.
En revanche, un risque élevé de méningiome a été observé lors de l’utilisation de doses élevées d’acétate de cyprotérone (ACP), un puissant progestatif ayant une activité antiandrogène, chez les femmes, les hommes et les transsexuels11-13.
De plus, l’arrêt d’un traitement à long terme par ACP induit une régression tumorale, ce qui a également été observé après l’arrêt de deux autres progestatifs puissants : l’acétate de nomégestrol (NOMAC) et l’acétate de chlormadinone (CMA)14-23, ce qui suggère que ces deux progestatifs sont également associés au risque de méningiome.
However, unlike ACP, no large -scale epidemiological study has yet been published on the risk of meningioma associated with exposure to the Nomac or CMA.
Nous avons donc cherché à évaluer, en situation réelle, l’association entre la chirurgie des méningiomes intracrâniens et l’exposition à trois puissants progestatifs pour lesquels une régression du volume du méningiome après l’arrêt du traitement a été décrite : ACP, NOMAC et CMA.
Methods
Data source
In this national case-to-test study based on the population, the data has been extracted from the National Health Data System (SNDS), which covers 99% of the population living in France-67 million residents. The SNDS includes demographic data, the dismissal of ambulatory drugs and information on hospital care (hospital diagnostic codes according to the international classification of diseases, tenth revision [CIM-10], and acts carried out during the hospital stay coded according to the medical classification of clinical acts [CCAM]).
These data are all prospectively recorded at the individual and anonymized level. This database is a useful and reliable source for the evaluation of the efficiency and safety of drugs24,25. This study was carried out within the framework of the regulatory decision of the French Agency for Data Protection CNIL-2016-316.
Case and witnesses
Les cas éligibles étaient tous les individus vivant en France et ayant subi une chirurgie pour méningiome intracrânien l entre le 1er janvier 2009 et le 31 décembre 2018 en France.
La chirurgie pour méningiome intracrânien était définie par la combinaison suivante enregistrée pour un même séjour hospitalier : un néoplasme de méningiome (codes CIM-10 : D32, D42 ou C70) codé comme diagnostic principal de l’hospitalisation et une intervention chirurgicale correspondant à une chirurgie intracrânienne (tableau supplémentaire 1).
The first surgical intervention for intracranial meningioma during the study period was included and the absence of a hospital stay for intracranial meningioma surgery since June 2007 has been verified. The index date has been defined as the date of admission to the hospital for a first meningioma surgery. For the sake of simplicity, the expression "surgery of intracranial meningioma" is designated below by the term "meningioma" in the results.
Five witness individuals have been paired with each case for the year of birth, sex at birth and the area of residence (100 geographic administrative zones), because age and sex are two major confusion factors in the association between exposure to progestins and meningioma. The witness individuals were selected randomly with at least one reimbursement of extrahospital care during the study period, excluding cases. The witnesses were awarded the same index date as their corresponding case and were alive on that index date.
Exposure
Pour les cas et les témoins, l’exposition à un progestatif a été définie comme au moins une délivrance de l’un des médicaments suivants (codés selon le système de classification anatomique thérapeutique chimique, ATC) au cours de l’année précédant la date d’index : ACP (G03HA01), NOMAC (G03DB04) et CMA (G03DB06).
ACP is a synthetic progestogen with anti-diandal activity indicated for inoperable prostate cancer or paraphilies in men (50-100 mg/day) and for various disorders of the spectrum of hirsutism or hyperandrogenism in women (50 mg/day). In addition, the ACP is used in an unauthorized manner as a feminizing hormone therapy for transsexuals. The ACP can also be used at a dose of 25 mg/day, because the tablets are divisible. Nomac (3.75-5 mg/day) is a synthetic progestogen prescribed mainly for HOS and contraception.
Finally, CMA (2-10 mg/day) is another progestogen indicated in the treatment of menstrual disorders, HOS, endometrial hyperplasia and endometriosis.
Nomac and CMA are not indicated for men in France.
Exposure to progestins has been defined using three indicators:
- - "The current use" has been defined as exposure to progestins with at least a delivery of the drug during the 365 days preceding the date of index, whether the subject has been exposed before or not;
- - "short -term use" as exposure to progestins during the 365 days preceding the index date, without exposure during the period between 366 and 730 days before the index date;
- - and "prolonged use" as exposure to progestins both during the 365 days preceding the index date and between 366 and 730 days before the index date, without taking into account the previous exposure.
We studied prolonged use by assessing exposure to progestins for the period 2013-2018, for which cases and witnesses had at least six years of history in the database. We have defined "prolonged use" as explained above for cases and witnesses and added five additional indicators of prolonged use: "prolonged use for two years" was defined as at least one of a progestogen per year for two years (that is to say before the 365 days preceding the date of the index and between 366 and 730 days before the date of the index, but not between 731 days and 1 096 days before date of index). "Prolonged use for three years", "four years", "five years" and "six years or more" were defined according to the same logic.
Covariable
La population étudiée a été décrite en fonction des caractéristiques socio-démographiques de base suivantes : sexe à la naissance, âge et zone de résidence (six groupes). Les informations sur les méningiomes comprenaient l’année de la chirurgie, le site anatomique (cinq sites principaux et 16 sites détaillés, décrits dans le tableau supplémentaire 1), le grade de la tumeur selon la CIM-10 et la radiothérapie associée à la chirurgie. La mortalité toutes causes confondues a été estimée à deux ans après la chirurgie du méningiome pour l’ensemble de la population des cas et à cinq ans pour le sous-ensemble des cas pour lesquels des données de suivi suffisantes étaient disponibles, c’est-à-dire pour ceux ayant subi une chirurgie du méningiome avant le 1er janvier 2016.
Statistical analyzes
The incidence rates of intracranial meningomes surgery per 100,000 people-years for the entire French population have been estimated by age class with the publicly available data from the National Institute of Statistics and Economic Studies. Logistic regression models packaged by paired pairs (to control the pairing variables) have been used to estimate the ODDS ratios (gold) and their confidence intervals (CI) at 95% for the association between meningioma and anterior exposure to progestins. The risk of meningioma associated with exposure to progestins has been estimated by considering either exposure to at least one of the three progestins, or each progestogen separately, depending on the current, short -term and prolonged use. The analyzes were then stratified by age group and sex, grade of the tumor and anatomical site. We also estimated the association between the NF2 (CIM-10 Q851 Code) and the meningioma to determine whether this well-documented association2 was also found in our studied population.
The fraction of cases attributable to the population was calculated from the gold obtained for global exposure, assuming adequate control of all confusion factors26,27. This attributable fraction was applied to the total number of cases during the study period to estimate the number of meningiomal cases attributable to the three powerful progestins, assuming a causal association between exposure to powerful progestins and meningioma. This estimate was also carried out for men and women separately. Finally, we estimated the number of cases of meningiomas attributable to the NF2.
Results
In total, 25,216 cases having undergone surgery for intracranial meningioma and 126,080 witness individuals were included (Figure 1).
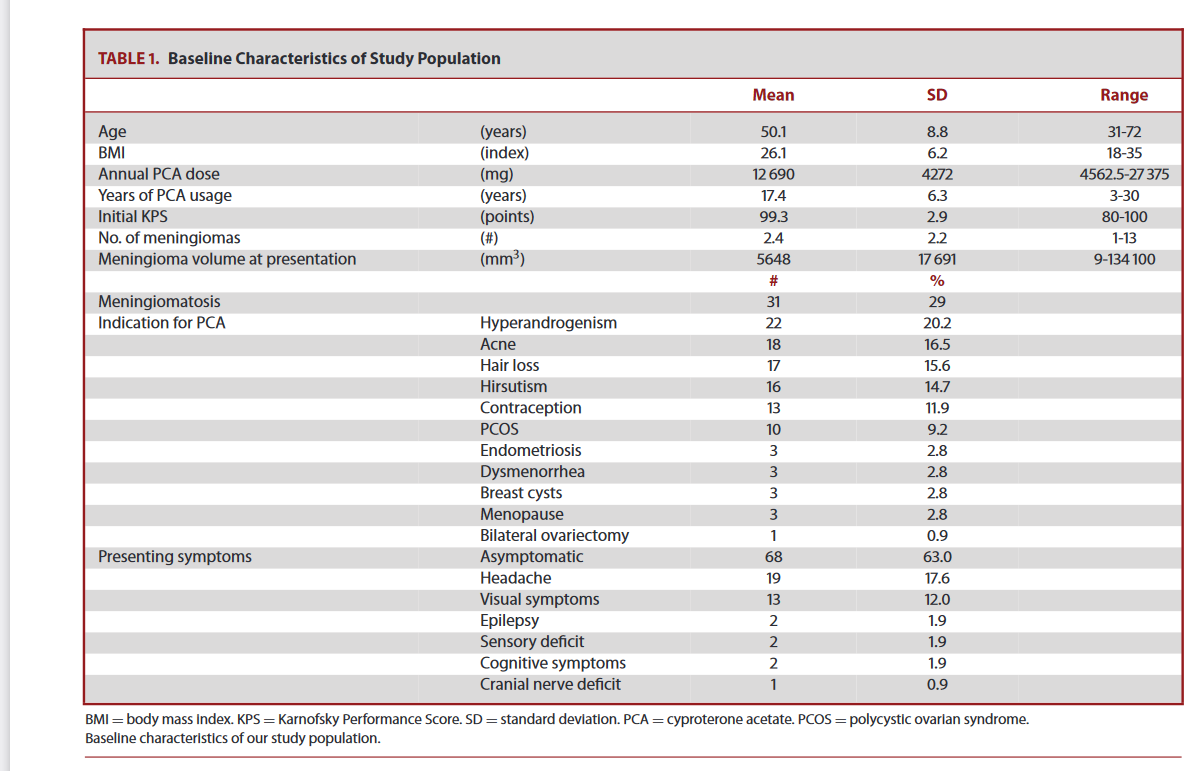
Their characteristics (women 75 %, median age: 58 years [Q1-Q3: 48-67]) are presented in Table 1.
The raw incidence of intracranial meningiomes surgery was 4/100,000 people-years, with a maximum woman/man ratio (4.6) reached between 45 and 54 years (Figure 2).
La plupart des méningiomes intracrâniens étaient situés dans la zone de convexité (37,9 %) et la base antérieure du crâne (20,9 %). Quatre-vingt-onze pour cent des tumeurs ont été classées comme bénignes (tableau 1).
About 7 % of patients died within five years of the operation, with higher mortality (25.5 %) for those with malignant tumors.
The current use of at least one of the progestins the year preceding the date of the index was found for 2,497 cases (9.9 %) and 2,382 (1.9 %) witnesses (Table 2). Most current progestogen users had prolonged use (91.8 % [2291/2497] in the case group and 63.9 % [1521/2382] in the control group).
For the subjects included in the period 2013-2018 with prolonged use of progestins, 79.0% of cases (1130/1430) and 43.4% of witnesses (392/903) had been exposed each year for at least six years (additional table 2). Cases and witnesses used doses of similar drugs (additional table 3): 50 mg for ACP (95 %), 5 mg for the nomac (86 %) and 10 mg for the CMA (81 %).
The estimated gold of meningioma for interest exposure are presented in Table 2. The NF2 was associated with an increased risk of meningioma: or = 19.5 [95%CI: 13.1-29,1]. Exposure to at least one of the progestins for current use, short-term use or prolonged use was associated with an increased risk of meningioma: or = 6.7 [6,3-7,1], 1.2 [1.0-1,4] and 9.5 [8,8-10,2], respectively. The extent of the risk has decreased between ACP, nomac and AMC: or = 22.7 [19.5-26.4], 6.5 [5,8-7,2] and 4.7 [4,5-5,3], respectively.
L’utilisation actuelle de progestatifs était associée à un risque de méningiome chez les femmes, avec un OR de 6,6 [6,3-7,1] (tableau 3 et tableau supplémentaire 4). Le RC diminuait de l’ACP à la NOMAC et à l’AMC : RC = 19,7 [17,0-22,7], 4,7 [4,3-5,1] et 3,3 [3,0-3,6], respectivement.
L’OR chez les hommes exposés uniquement à l’ACP était de 8,0 [5,2-12,3]. L’ampleur de l’association augmentait avec l’âge chez les femmes mais diminuait chez les hommes. L’exposition à un progestatif a été associée à un risque accru de méningiome chez les femmes pour les tumeurs bénignes, atypiques et malignes : OR=6,6 [6,2-7,1], 7,0 [5,4-9,1] et 6,6 [4,0-10,8], respectivement.
Exposure to a progestogen was also significantly associated with mild and atypical meningiomas in men.
Les sites anatomiques pour lesquels le risque de méningiome associé aux progestatifs était le plus élevé étaient la base antérieure et moyenne du crâne : OR=10,2 [8,9-11,6] et 9,7 [8,6-11,1] respectivement, pour tous les progestatifs ; OR=35,7 [26,5-48,2] et 23,9 [17,8-32,2] respectivement, pour l’ACP ; OR=6. 2 [5,2-7,4] et 6,8 [5,7-8,1], respectivement, pour le NOMAC ; et OR=3,5 [2,9-4,4] et 4,7 [3,9-5,7], respectivement, pour l’AMC (Tableau 3). Après une évaluation plus précise de cette association par site anatomique (tableau supplémentaire 5 et tableau supplémentaire 6), les sites présentant les OR les plus élevés étaient la zone optochiasmatique (OR=12,6 [10,0-15,8]) et le tiers médial de la base du crâne moyen impliquant l’angle sphéno-orbitaire (OR=12,0 [10,2-14,1]). Le risque associé à l’ACP était particulièrement élevé pour la zone optochiasmatique (OR=49,1 [28,9-83,5]).
La fraction attribuable à la population (FAP) de méningiomes traités chirurgicalement pour une utilisation actuelle d’au moins un des trois progestatifs puissants étudiés en France entre 2009 et 2018 était de 8,4% [8,0-8,8%]. Le nombre correspondant de méningiomes attribuables était de 2 124 [2008-2020] (212 par an, en moyenne), en supposant l’hypothèse d’une association causale entre l’exposition aux progestatifs puissants et le méningiome.
The FAP des Méningiomes was 11.0% [10.5-11.5%] for women and 0.8% [0.5-1.0%] for men, with a corresponding number of attributable cases of 2072 [1978-2165] and 48 [33-63].
The meningioma FAP for the NF2 was 0.4% [0.3-0.5%] and the estimated number of attributable meningiomas was 111 [90-132].
Discussion
Cette étude a révélé une forte association entre les méningiomes intracrâniens nécessitant une intervention chirurgicale et l’exposition prolongée à des progestatifs puissants, avec un gradient croissant de l’AMC au NOMAC et à l’ACP.
Cette augmentation du risque concernait tous les grades et tous les sites anatomiques mais était la plus élevée pour la base du crâne antérieure et moyenne pour chaque progestatif. Le nombre estimé de cas attribuables aux progestatifs puissants était supérieur à 2 000 en France entre 2009 et 2018, soit environ 20 fois celui des cas attribuables à la NF2.
Our results showing a strong association between long exposure to ACP and the risk of operated meningioma (or = 22.7 [19.5-26.4]) are in accordance with those of other studies. A strong dose-answer relationship between ACP and intracranial meningiomas has already been reported in women in France (HR = 21.7 [10.8-43.5] for cumulative doses> 60g) 13, in men in Denmark (HR = 18.5 [9,2-37,1] for cumulative doses> 10g) 28, and in transsexuals standardized incidence: 11.9 [5.5-22.7]) 12.
On the other hand, no epidemiological study published to date has shown an association between exposure to the CMA or the nomac and the meningiomas. Meningioma cases have been published for the Nomac18,19 and the CMA16 or included in larger series including ACP20,29. Several years long exposure, locations at the base of the skull (frequently with ophthalmological symptoms), and non -systematic regression when you stop treatment in the absence of surgery have been reported.
Dans une revue récente, Hage et al. ont montré que les preuves actuelles de l’association entre THS et méningiome sont contradictoires, mais semblent favoriser un risque accru10. Deux études de cohorte non publiées sur l’AMC et le NOMAC sont en cours de discussion à l’Agence européenne du médicament30.
In our study, we found a significant association between the prolonged use of the AMC and the nomac, although the gold are lower than those of the ACP. Results as diverse for the association between meningioma and progestins probably reflect the use of different types of progestins and prolonged use and the high dose seeming to contribute to the association with meningioma. In particular, the use of these three progestins (ACP, CMA and Nomac) in France has been higher in terms of frequency and dose than in other countries of Western Europe. ACP, CMA and Nomac are not currently marketed in the United States. Such an association between powerful progestins and meningiomas could therefore not be demonstrated in the past in the United States.
Nous avons constaté que le risque de méningiome opéré était le plus élevé dans la partie antérieure et moyenne de la base du crâne chez les patientes exposées aux progestatifs. Ce résultat est cohérent avec ceux des études observationnelles précédentes et avec les mécanismes biologiques connus.
In a study on 300 patients who have undergone surgery for meningioma, a higher rate of expression of progesterone receptors> 50% was observed for meningiomas of the median skull base than for other sites 7.
En outre, les méningiomes associés à la progestérone présentaient des niveaux significativement plus élevés d’expression des récepteurs de la progestérone et étaient plus fréquemment situés à la base du crâne que les autres méningiomes 8
Another specific characteristic of meningiomas associated with progestins are mutations affecting the PIK3CA/AKT1 track, which have been more frequently observed in the ACP meningiomas than in a control group8,21.
Such a preferential mutational landscape of meningiomas induced by the ACP seems to have been confirmed by an observational study showing the coexistence of meningiomas in regression bearing a PIK3CA mutation and growing meningiomas carrying NF2 mutations in the same patient after stopping the drug in four women exposed to ACP21.
An independent clonal origin, associated with a predisposition of certain meningeal cells (mainly located in the anterior and average skull) to develop meningiomas, could explain the pathogenesis of these meningiomas linked to progestins21.
Une étude épidémiologique française a également rapporté que le risque de méningiome de la base antérieure du crâne était 47 fois plus élevé chez les patients exposés à l’ACP13. De manière intéressante, nous avons mis en évidence une forte association avec les méningiomes de la base du crâne médiane impliquant l’angle sphéno-orbitaire (OR=12,0 [10,2-14,1]). Une seule étude antérieure s’est intéressée à ce site spécifique et a constaté qu’une forte proportion de femmes présentant de telles tumeurs avaient été exposées à de fortes doses d’ACP, NOMAC ou CMA pendant au moins deux ans29. De plus, nos résultats ont montré que le risque accru concerne les méningiomes opérés de tous les grades. Bien que des rapports de cas et des séries de cas de méningiomes de grade 2 associés à l’ACP, NOMAC ou CMA aient été publiés, aucune preuve épidémiologique d’un risque accru n’était disponible jusqu’à présent23.
Strengths of this study
La principale force de l’étude était la conception basée sur les registres et la taille de la population (plus de 25 000 chirurgies pour méningiome sur 10 ans et 125 000 contrôles). L’utilisation d’enregistrements prospectifs des médicaments délivrés dans le SNDS a permis d’éviter le biais de rappel, une limite majeure des études cas-témoins. De plus, nous pouvons souligner l’exactitude des données sur l’exposition aux progestatifs et la localisation des méningiomes opérés selon la procédure chirurgicale. Nous avons également calculé les fractions attribuables à la population, ce qui permet de soutenir l’évaluation de la charge de morbidité d’un facteur causal dans une population.
Our short -term approach (<1 year) vs long term (> 1 year) highlighted the absence of risk or a very small risk with short -term use for each of the three powerful progestins. The risk of meningioma is mainly linked to very long -term use (> 5 years), which has not been assessed in previous studies.
Limits of this study
Premièrement, nous avons inclus des patients qui ont subi une chirurgie pour un méningiome intracrânien, alors qu’une radiothérapie exclusive est également indiquée. Cependant, la chirurgie est la première option pour la gestion des méningiomes de tout grade 31. Dans une étude française, seuls 4 % des patients ayant développé un méningiome après une exposition à l’ACP ont été traités par radiothérapie 13.
We have included patients who have undergone surgery, regardless of the grade of the tumor. The classification of tumors did not precisely follow the last classification of the grades of WHO 32 due to the source of the data, but the CIM-10 codes were reliable because they were recorded by the surgeons. As expected, mortality and radiotherapy rates associated with surgery increased with the rank of the tumor in our study.
Anatomical sites have been classified according to information available using the French medical classification of clinical acts. Different classifications have been used in previous studies, no consensual surgical anatomical classification being currently available. Our classification made it possible to consider a large number of sites (16 groups). In addition to diagnostic codes, clinical procedures are recorded by surgeons and can therefore be considered reliable.
En termes d’exposition, l’indication du traitement progestatif n’était pas disponible. Cependant, les trois progestatifs ont, en partie, des indications différentes et ont tous été associés à un risque accru de méningiome. Toutes les tranches d’âge étaient concernées par ce risque accru et il n’y avait pas de risque différentiel d’ACP pour les hommes, les femmes ou les transsexuels. L’indication n’est donc pas susceptible d’être un facteur de confusion dans l’évaluation du risque de méningiome associé aux progestatifs. En ce qui concerne la durée d’exposition, nous avons considéré l’utilisation actuelle, même si le méningiome est généralement une tumeur à croissance lente. Malgré cette limitation, nous montrons une association significative, en particulier pour une utilisation prolongée (>1 an). Nous avons émis l’hypothèse que l’utilisation prolongée reflète une plus longue durée d’exposition aux progestatifs, avec la prescription, l’administration et la prise répétées de médicaments. La description de l’exposition prolongée pour la période 2013-2018 tend à confirmer cette hypothèse : 80% de l’utilisation prolongée correspondait à une exposition chaque année pendant au moins les six années précédant la date d’index. Nous n’avons pas évalué l’effet de l’arrêt du traitement progestatif. Plusieurs études ont conclu que l’arrêt de l’ACP, du NOMAC ou de l’AMC entraînait une diminution du risque de méningiome ou une régression tumorale13-19. Nous n’avons pas tenu compte des radiations ionisantes, car ce facteur de risque ne s’applique qu’à quelques cas33,34 et il est peu probable qu’il confonde l’exposition aux progestatifs.
Enfin, nous ne pouvons pas formellement exclure la possibilité que l’indication de la chirurgie pour les patientes exposées ait changé au fil du temps. L’étiquetage de l’ACP a été modifié en 2011 et 2013 pour fournir des informations sur les cas de méningiome signalés associés à l’utilisation du médicament. Néanmoins, ces mises à jour ont eu peu d’impact sur les soins cliniques 13 et nous avons supposé que le choix de la prise en charge neurochirurgicale était basé sur les directives européennes actuelles pour la plupart des cas et que les patients asymptomatiques étaient pris en charge par observation. L’étiquetage de l’AMC et du NOMAC a été modifié en 2018, c’est-à-dire au cours de la dernière année de la période d’étude.
Clinical implications and future research
In France, the screening of meningiomas by magnetic resonance imaging in patients receiving progestogen for long -term treatment has already been set up for ACP and will soon be recommended for AMC and Nomac 35.36. People who have used powerful progestins for many years could benefit from such screening. Future research could explore the association between very long -term exposure to low -dose progestoges contained in oral contraceptives and the risk of meningioma.
Conclusion
In this case-control study at the national level, we observed a strong and significant association between exposure to three progestins and meningioma surgically treated. The risk was high for patients with prolonged use and for meningiomas operated on the previous base and average of the skull.
L’ablation chirurgicale de ces tumeurs est l’une des formes les plus difficiles de chirurgie intracrânienne et est associée à un risque beaucoup plus élevé. Nos données devraient encourager l’information des personnes utilisant des progestatifs puissants pendant des périodes prolongées sur ce risque et l’évaluation du rapport bénéfice/risque individuel.
Regulatory and ethical aspects
The French public establishment carrying out this study, the EPI-Phare scientific interest group, has permanent access to the SNDS database in accordance with the provisions of articles R.1461-12 and following of the Code of Public Health and the Decision of the National Commission for Data Protection CNIL-2016-316. This study was recorded in the study register of the EPI-Phare scientific interest group. No informed consent was therefore required. This research did not benefit from any specific funding.
Data availability
Data sharing is not applicable. In accordance with French laws governing data protection and French regulations, the authors cannot publicly disseminate data from the National Health Data System (SNDS). However, any person or structure, public or private, for profit or not, can access SNDS data on authorization from the National Commission for Computer Science and Liberties (CNIL) to carry out a study, research or evaluation of public interest (https://www.snds.gouv.fr/snds/procus-d-acces-aux-donnees and https://www.snds.gouv.fr).
Funding
No funding was received for this work.
Competing interests
The authors do not report any competitive interest.
References
- Ostrom QT, Cooffi G, Waite K, Kruchko C, Barnholtz-Sloan JS. CBTRUS Statistical Report:
Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in
2014-2018. Neuro Oncol. 2021 Oct 5; 23 (supplement_3): III1–105.
- Wiemels J, Wrensch M, Claus EB. Epidemiology and Etiology of Meningioma. J Neurooncol.
2010 Sep; 99 (3): 307–14.
- Casabella am, Urakov TM, Basil G, MORCOS JJ. Management of Foramen Magnum Meningioma
During pregnancy: Literature Review and Case Report. World Neurosurg. 2017 Jan; 97: 752.e15-
752.E18.
- Chakravarthy V, Kaplan B, Gospodarev V, Myers H, Los Reyes K, Achiriloaie A. Houdini
TUMOR: CASE Report and literature Review of pregnancy-associated meningioma. World
Neurosurg. 2018 Jun; 114: E1261–5.
- Omuglecka A, Paperz W, Nawrocka-Kunecka A, Lewy-Trenda I. Immunohistochemical
Expression of Progesterone and Estrogen Receptors in Meningiomas. Folia Neuropathol.
2006;44(2):111–5.
- Ülgen e, bektaşoğlu pk, sav ma, can Ö, danyeli ae, hızal db, et al. MENINGIOMAS DISPLAY A
Specific immunoxpression pattern in a rostrocaudal gradient: an analysis of 366 patients.
World Neurosurg. 2019 Mar; 123: E520–35.
- Maiuri F, Mariniello G, Guadagno E, Barbato M, Corvino S, Del Basso de Caro M. Who
grade, proliferation index, and progesterone receptor expression are different according to the
rental of meningioma. Acta Neurochir (Wien). 2019 DEC; 161 (12): 2553–61.
- Peyre M, Gaillard S, de Marcellus C, Giry M, Bielle F, Villa C, et al. Progestin-associated shift
of Meningioma Mutational Landscape. Ann Oncol. 2018 01; 29 (3): 681–6.
- Michaud DS, Gallo V, Schlehofer B, Tjønneland A, Olsen A, Overvad K, et al. Reproductive
factors and exogeunous hormone use in relationship to risk of glioma and meningioma in a large
European Cohort Study. Epidemiol cancer Biomarkers Prev. 2010 Oct; 19 (10): 2562–9.
- Hage M, Plesa O, Lemaire I, Raffin Sanson ML. Estrogen and Progesterone Therapy and
Meningiomas. Endocrinology. 2022 Feb 1; 163 (2): Bqab259.
- Gil M, Oliva B, Timoner J, Maciá Ma, Bryant V, de Abajo fj. Risk of Meningioma Among
Users of High Doses of Cyproterone Acetate AS Compared With the General Population: Evidence
from a population-based cohort study. BR J FLUS PHARMACOL. 2011 Dec; 72 (6): 965–8.
- Note nm, wiepjes cm, from Blok CJM, Gooren LJG, Peerdeman SM, Kreukels BPC, et al. Tea
occurrence of benign brain tumours in transgender individuals during cross-sex hormone
Treatment. Brain. 2018 Jul 1; 141 (7): 2047–54.
- Weill A, Nguyen P, Labidi M, Cadier B, Passeri T, Duranteau L, et al. Use of High Dose
Cyproterone Acetate and Risk of Intracranial Meningioma in Women: Cohort Study. BMJ. 2021 Feb
3; 372: N37.
- Bernat al, oyama k, hamdi s, mandonnet e, vexiau d, pocard m, et al. Growth Stabilization
and regression of meningiomas after discontinuization of cyproterone acetate: a case series of 12
Patients. Acta Neurochir (Wien). 2015 Oct; 157 (10): 1741–6.
- Voormolen ehj, champagne po, roca e, giammattei l, passi t, di russo p, et al.
Intracranial meningiomas Decrease in Volume on Magnetic Resonance Imaging After
Discontinuing progestin. Neurosurgery. 2021 Jun 24; nyab175.
- Shimizu J, Matsumoto M, Yamazaki E, Yasue M. Spontaneous Regression of an Asymptomatic
Meningioma Associated with Discontinuization of Progesterone Agonist Administration. Neurol med
Chir (Tokyo). 2008 May; 48 (5): 227–30.
- Vadivelu s, shaore L, Schulder M. Regression of Multiple Intracranial Meningiomas After
Cessation of Long-Term Progesterone Agonist Therapy. J neurosurg. 2010 May; 112 (5): 920–4.
- Passeri T, Champagne Po, Bernat Al, Hanakita S, Hall H, Mandonnet E, et al. Spontaneous
Regression of meningiomas after interruption of numegestrol acetate: a series of three patients.
Acta Neurochir (Wien). 2019; 161 (4): 761–5.
- Champagne Po, Passeri T, Froelich S. Combined Hormonal Influence of Cyproterone Acetate and Numegestrol Acetate on Meningioma: a case report. Acta Neurochir (Wien). 2019; 161 (3): 589–92.
- Malaize H, Samoyeau T, Zanello M, Roux A, Benzakoun J, Peeters S, et al. Evolution of the
Neurosurgical Management of progestin-associated meningiomas: A 23-Year Single-Center
experience. J Neurooncol. 2021 apr; 152 (2): 279–88.
- Passeri T, Giammattei L, the van T, Abbritti R, Perrier A, Wong J, et al. Atypical Evolution of
meningimatosis after discontinuation of cyproterone acetate: clinical boxes and histomolecular
Characterization. Acta Neurochir (Wien). 2021 Oct 6;
- Devalckeneer A, Aboukais R, bourgeois P, de Witte O, Racape J, Caron S, et al. Prelination
Report of Patients With Meningiomas Exposed to Cyproterone Acetate, Nomegestrol Acetate and
Chlormadinone Acetate - Monocentric Ongoing Study on Progestin Related Meningiomas. Wink
Neurosurg neurol. 2021 Nov; 210: 106959.
- DEVALCKENEER A, Aboukais R, making M, bourgeois P, Quentin VM, Maurage CA, et al.
Progestin-Related who Grade II Meningiomas Behavior-A Single-Institution Comparative Case
series. Neurosurg Rev. 2021 Nov 30;
- Weill A, Dalichampt M, Raguideau F, Ricordeau P, Blotière Po, Rudant J, et al. Low dose
OESTROGEN Combined Oral Contraception and Risk of Pulmonary Embolism, Stroke, and Myocardial
Infarction in Five Million French Women: Cohort Study. BMJ. 2016 10; 353: I2002.
- Lemaitre M, Kirchgesner J, Rudnichi A, Carrat F, Zureik M, Carbonnel F, et al. Association
Between use of thiopurines or tumor necrosis factor antagonists alone or in combination
and risk of lymphoma in patients with inflammatory bowel disease. Jama. 2017 Nov
7;318(17):1679–86.
- Rothman KJ, Greenland S, Lash tl. Modern Epidemiology. Lippincott Williams & Wilkins;
- 776 p.
- Greenland S. Bias in Methods for deriving standardized morbidity ratio and attributable estimates fraction. Stat Med. 1984 Jun; 3 (2): 131–41.
- Mikkelsen AP, Greiber Ik, Scheller Nm, Hilden M, Lidegaard Ø. Cyproterone Acetate and Risk
Of Meningioma: A Nationwide Cohort Study. J neurol neurosurg psychiatry. 2021 Jun 29; Jnnp-
2021-326138.
- APRA C, Roblot P, Alkhayri A, Le Guérinel C, Polivka M, Chauvet D. Female Gender and
Exogenous progesterone exhibition as risk factors for spheno-organ meningiomas. J
Neurooncol. 2020 Aug; 149 (1): 95–101.
- [CITED 2020 Jun 17]. Available from: http: // Agencyprd.
ANSM.SANTE.fr/php/ecodex/frames.php?Specid=62673690&typedoc=r&ref=R0332273.htm
- Goldbrunner R, Minniti G, Preusser M, Jenkinson MD, Sallabanda K, Houdart E, et al. Eano
Guidelines for the Diagnosis and Treatment of Meningiomas. Lancet Oncol. 2016 Sep; 17 (9): E383-
391.
- Louis Dn, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, et al.
The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A
Summary. Acta Neuropathol. 2016 Jun; 131 (6): 803–20.
- Taylor AJ, Little MP, Winter DL, Sugden E, Ellison DW, Stiller Ca, et al. Population-based
Risks of CNS Tumors in Survivors of Childhood Cancer: The British Childhood Cancer Survivor
Study. J Clin Oncol. 2010 Dec 20; 28 (36): 5287–93.
- Braganza Mz, Kitahara CM, Berrington de González A, Inskip PD, Johnson Kj, Rajaraman P.
Ionizing Radiation and the Risk of Brain and Central Nervous System Tumors: A Systematic Review.
Neuro Oncol. 2012 Nov; 14 (11): 1316–24.
- News - Cyproterone (Androcur, Diane 35, and generics) and vasoconstrictors acetate
(pseudoephedrine): return of information on the PRAC of February 2020 - ANSM [Internet]. [CITED
2021 Jun 28]. Available from: https://ansm.sante.fr/actualites/acetate-de-cyproterone-androcurdiane-
35-and-generics and vasocstrractors-pseudoephedrine-return-Dinformation-sur-le-Pracde-
February-2020
- News - Lotényl and Lotéran: upcoming documents to strengthen patient information - ANSM [Internet]. [CITED 2021 Jun 28]. Available from: https://ansm.sante.fr/actualites/lutenyl-etluteran-documents-ave-venre-renfrofer-linformation-des-Patients
Figures
Figure 1 Organization chart
Figure 2 Incidence of meningiomas treated surgically depending on the age group and sex at birth
Paintings
Table 1. Characteristics of case and control groups
CIM-10: International classification of diseases, tenth revision; Sex, woman: individuals born women
† Northeast: Grand Est, Bourgogne Franche-Comté, Hauts-de-France; Paris region (Ile-de-France): City of Paris and Île-de-France region; North-West: Brittany, Val de Loire center, Normandy, Pays de la Loire; South-East: Auvergne-Rhône-Alpes, Provence-Alpes-Côte d'Azur, Corsica; Sud-Ouest: Nouvelle-Aquitaine, Occitanie; Overseas zone: Guadeloupe, Martinique, Guyana, meeting
‡ Death within 2 years: for the whole cohort, the deaths all causes have been identified from the date of indexing up to 2 years after this date.
- Death within 5 years: The deaths of all causes were identified from the index date up to 5 years later for all cases having undergone meningioma surgery before January 1, 2016.
Table 2. Nudes and proportions of cases and witnesses exposed and estimated, taking into account the match variables, with confidence intervals
However: Odds Ratio, by controlling the pairing factors (sex at birth, year of birth and area of residence).
Current use: Exhibition at least once within 365 days preceding the date of the index, regardless of previous exposure; Short -term use: exposure within 365 days of the date of the index, excluding the period between 365 and 730 days before the date of the index; Prolonged use: Exhibition both within 365 days and between 365 and 730 days before the index date
Table 3. Association between meningioma surgically treated and exposure to progestins depending on age, sex at birth, grade and the site of the tumor; Estimated and 95%IC.
However: Odds Ratio, by controlling the pairing factors (sex at birth, year of birth and region of residence)
CIM-10: International classification of diseases, tenth revision; Sex, feminine: individuals born of female sex
Table 1. Characteristics of case and control groups
Characteristics Case controls
N = 25.216 n = 126.080
n (%) n (%)
Sex (birth)/Woman 18.892 (74.9) 94,460 (74.9)
Age, average (sd) 57.5 (13.5) 57.5 (13.5)
Age group
0-19 128 (0.5) 640 (0.5)
20-34 1,021 (4.1) 5,105 (4.1)
35-44 3,132 (12.4) 15,660 (12.4)
45-54 6,132 (24.3) 30,660 (24.3)
55-64 6,552 (26.0) 32,760 (26.0)
65-74 5,570 (22.1) 27,850 (22.1)
75-84 2,421 (9.6) 12,105 (9.6)
≥ 85 260 (1.0) 1,300 (1.0)
Zone of residence †
Paris region 4,331 (17.2) 21.655 (17.2)
Northeast 4,842 (19.2) 24,210 (19.2)
North West 5,000 (19.8) 25,000 (19.8)
South-East 5.755 (22.8) 28,775 (22.8)
South West 4,802 (19.0) 24.010 (19.0)
Overseas 486 (1.9) 2.430 (1.9)
Year of operation
2009 2,070 (8.2)
2010 2,220 (8.8)
2011 2,299 (9.1)
2012 2,464 (9.8)
2013 2,469 (9.8)
2014 2,639 (10.5)
2015 2,628 (10.4)
2016 2,762 (10.9)
2017 2,742 (10.9)
2018 2,923 (11.6)
Anatomical location of meningioma
Anterior skull base 5.285 (20.9) -
Average skull base 4.790 (19.0)
Posterior base of the skull 2.770 (11.0)
Convexity 9.554 (37.9)
Falx and Tentorium 2.608 (10.3)
Other places 209 (0.8)
Grade of the ICD-10 tumor
Benin (D32) 23.010 (91.3)
Sex, woman 17,429 (75.7)
Atypical (D42) 1.587 (6.3)
Sex, woman 1.101 (69.4)
Malin (C70) 619 (2.4)
Sex, woman 362 (58.5)
Adjuvant radiotherapy
All grades 2.274 (9.0)
Benin (D32) 1,917 (8.3)
Atypical (D42) 145 (9.1)
Malin (C70) 212 (34.2)
Death, according to the rank of the tumor, in
2 ans (N=25216) ‡
All grades 854 (3.4)
Benin (D32) 692 (3.0)
Atypical (D42) 70 (4.4)
Malin (C70) 92 (14.8)
5 ans (N=16789) §
All grades 1,152 (6.8)
Benin (D32) 971 (6.3)
Atypical (D42) 91 (8.5)
Malin (C70) 90 (25.5)
CIM-10: International classification of diseases, tenth revision; Sex, woman: individuals born of female sex.
† North East: Grand Est, Bourgogne Franche-Comté, Hauts-de-France; Paris region (Ile-de-France): Paris and Ile-de-France region; North-West: Brittany, Val de Loire center, Normandy, Pays de la Loire; South-East: Auvergne-Rhône-Alpes, Provence-Alpes-Côte d'Azur, Corsica; Sud-Ouest: Nouvelle-Aquitaine, Occitanie; Overseas: Guadeloupe, Martinique, Guyana, Reunion
‡ Death within 2 years: for the entire cohort, the deaths all causes were identified for the date of index up to 2 years after this date.
- Décès dans les 5 ans : les décès, toutes causes confondues, ont été identifiés à partir de la date d’indexation jusqu’à 5 ans plus tard pour tous les cas ayant subi une chirurgie du méningiome avant le 1er janvier 2016.
Table 2. Nudes and proportions of exposed cases and estimated gold, by controlling the matching variables, with confidence intervals
Exhibition boxes controls or [95% CI]
N = 25.216 n = 126.080
Neurofibromatosis Type II 117 (0.5) 30 (0.02) 19.5 [13.1-29.1]
Exposure to at least one of the progestins
Current use 2.497 (9.9) 2.382 (1.9) 6.7 [6.3-7.1]
Short term <1 year 206 (0.8) 861 (0.7) 1.2 [1.0 - 1.4]
Prolonged ≥ 1 year 2,291 (9.1) 1.521 (1.2) 9.5 [8.8 - 10.2]
Cyproterone acetate
Current use 961 (3.8) 290 (0.2) 18.3 [16.0-21.1]
Short term <1 year 30 (0.1) 63 (0.05) 2.4 [1.5-3.7]
Prolonged ≥ 1 year 931 (3.7) 227 (0.2) 22.7 [19.5-26.4]
Nomestrol acetate
Current use 969 (3.8) 1.149 (0.9) 4.7 [4.3-5.1]
Short term <1 year 105 (0.4) 421 (0.3) 1.3 [1.0-1.6]
Prolonged ≥ 1 year 864 (3.4) 728 (0.6) 6.5 [5.8-7.2]
Chlormadinone acetate
Current use 683 (2.7) 1.096 (0.9) 3.3 [3.0-3.6]
Short term <1 year 80 (0.3) 416 (0.3) 0.9 [0.8-1.2]
Prolonged ≥ 1 year 603 (2.4) 680 (0.5) 4.7 [4.5-5.3]
However: Odds Ratio, by controlling the pairing factor (sex at birth, birth year and area of residence)
Current use: exposure at least once within 365 days preceding the index date, regardless of previous exposure; Short -term use: exposure within 365 days preceding the index date, excluding the period between 365 and 730 days before the index date; Prolonged use: Exhibition both within 365 days and between 365 and 730 days before the index date
Table 3. Association between meningioma surgically treated and exposure to progestins depending on age, sex at birth, grade and the site of the tumor; Estimated but 95% IC
Exhibition one of 3 acetate of acetate of acetate of
Cyproterone Progestatives Nomegestrol Chlormadinone
Sex, woman
Global 6.6 [6.3-7.1] 19.7 [17.0-22.7] 4.7 [4.3-5.1] 3.3 [3.0-3.6]
0-19 5.0 [0.3-79.9] 5.0 [0.3-79.9] – –
20-34 5.4 [4.0-7.2] 12.6 [8.0-19.8] 3.1 [1.8-5.5] 2.0 [1.1-3.5]
35-44 6.0 [5.2-6.8] 21.9 [16.4-29.2] 3.5 [2.9-4.3] 2.6 [2.1-3.3]
45-54 6.3 [5.8-6.9] 18.7 [15.0-23.4] 4.6 [4.1-5.2] 3.6 [3.2-4.0]
55-64 8.9 [7.5-10.6] 21.8 [14.8-32.0] 7.1 [5.5-9.0] 4.1 [3.0-5.7]
≥ 65 years 10.6 [7.7-14.6] 27.9 [15.1-51.6] 7.7 [4.8-12.3] 1.8 [0.7-4.5]
Sex, man
Global 8.0 [5.2-12.3] 8.0 [5.2-12.3]
<65 years 12.5 [5.5-28.4] 12.5 [5.5-28.4]---
≥ 65 years 6.6 [4.0-11.0] 6.6 [4.0-11.0]---
ICD-10 grade tumor
Benin (D32) 6.7 [6.2-7.1] 18.4 [15.9-21.2] 4.7 [4.3-5.1] 3.3 [3.0-3.6]
Sex, woman 6.6 [6.2-7.1] 19.5 [16.7-22.7] 4.7 [4.3-5.1] 3.3 [3.0-3.6]
Sex, man 9.1 [5.7-14.6] 9.1 [5.7-14.6]---
Atypical (D42) 7.1 [5.5-9.2] 21.6 [12.1-38.6] 4.6 [3.2-6.7] 3.3 [2.2-4.9]
Sex, woman 7.0 [5.4-9.1] 21.7 [11.9-39.7] 4.6 [3.2-6.7] 3.3 [2.2-4.9]
Sex, man 20.0 [2.2-178.9] 20.0 [2.2-178.9]---
Malin (C70) 6.1 [3.8-9.8] 14.3 [6.0-33.8] 4.9 [2.2-10.8] 2.8 [1.3-5.9]
Sex, woman 6.6 [4.0-10.8] 23.7 [8.1-69.8] 4.9 [2.2-10.8] 2.8 [1.3-5.9]
Sex, man 1.7 [0.2-16.0] 1.7 [0.2-16.0]---
Anatomical location
Anterior skull base 10.2 [8.9-11.6] 35.7 [26.5-48.2] 6.2 [5.2-7.4] 3.5 [2.9-4.4]
Average skull base 9.7 [8.6-11.1] 23.9 [17.8-32.2] 6.8 [5.7-8.1] 4.7 [3.9-5.7]
Posterior base of the skull 2.9 [2.4-3.6] 6.4 [3.9-10.4] 2.6 [1.9-3.5] 2.1 [1.5-2.9]
Convexity 5.1 [4.6-5.7] 12.4 [9.9-15.5] 3.5 [3.0-4.2] 2.9 [2.4-3.4]
Falx and Tentorium 3.5 [2.8-4.5] 10.4 [6.2-17.4] 2.8 [1.9-3.9] 2.0 [1.3-3.0]
However: Odds Ratio, by controlling the pairing factors (sex at birth, year of birth and area of residence)
CIM-10: International classification of diseases, tenth revision; Female sex: people born of female sex
See diagram in the original document